Lacrimal System Anatomy
The lacrimal system has two parts: the secretory system (lacrimal gland — which produces tears) and the excretory system (drainage pathway — which carries tears from the eye to the nose). Understanding both is essential for diagnosing and treating tearing disorders, blocked ducts, and lacrimal infections.
Overview
Tear production begins at the lacrimal gland in the superolateral orbit. Tears flow across the ocular surface, propelled by blinking, and drain medially through the lacrimal drainage system into the nasal cavity. The entire pathway — from punctum to nasal meatus — spans only about 30 mm, but obstruction at any point causes epiphora (overflow tearing).
The tear film itself has three layers: a lipid layer (from Meibomian glands), an aqueous layer (from lacrimal and accessory glands), and a mucin layer (from goblet cells). Dysfunction of any layer — or obstruction of drainage — presents as tearing, irritation, or recurrent infection.
Lacrimal Gland
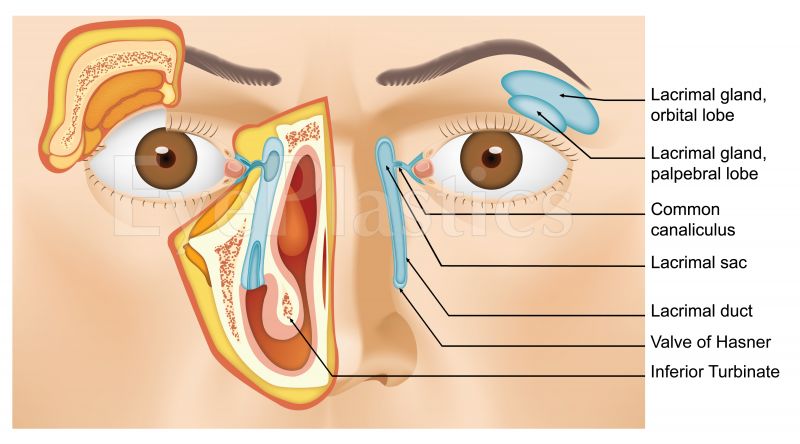
The lacrimal gland sits in the superolateral orbit within the lacrimal gland fossa of the frontal bone. It is divided by the levator aponeurosis into two lobes:
Orbital Lobe
Larger; sits behind the orbital septum. Not visible on eyelid eversion. Should not be biopsied or resected without careful consideration — doing so can significantly reduce tear production.
Palpebral Lobe
Smaller; visible in the superolateral conjunctival fornix when the upper eyelid is everted. The excretory ducts (6–12 ducts) from both lobes drain into the superior fornix 5 mm above the superior tarsal border.
Reflex tearing (from irritation, emotion) is mediated by the lacrimal gland via the facial nerve (CN VII parasympathetics). Basal tear secretion comes mainly from accessory glands — the glands of Krause (in the fornix) and Wolfring (above the tarsus) — which function without neural control.
Drainage Pathway — Overview
- 1Puncta
Two small openings on the medial upper and lower lid margins, sitting in the tear lake. Each is about 0.3 mm in diameter, elevated on a small papilla.
- 2Canaliculi
Each punctum leads to a vertical ampulla (2 mm), then a horizontal canaliculus (8–10 mm) running medially. In 90% of people, the superior and inferior canaliculi join to form a common canaliculus before entering the lacrimal sac.
- 3Lacrimal Sac
A small (12 mm tall) reservoir in the lacrimal sac fossa between the anterior and posterior limbs of the medial canthal tendon. The common canaliculus enters at a posterior-superior angle.
- 4Nasolacrimal Duct
The bony canal (12 mm long) descending from the lacrimal sac into the inferior nasal meatus, where tears drain beneath the inferior turbinate through the valve of Hasner.
Puncta & Canaliculi
The puncta sit approximately 6 mm from the medial canthus on the lid margin — the upper punctum slightly more medial than the lower. They are normally turned inward against the globe so they sit in the tear lake. Punctal eversion (common with lower lid laxity) displaces them away from the tear film, impairing drainage and causing tearing.
The canaliculi are surrounded by elastic fibers and expand slightly with the lacrimal pump. The valve of Rosenmüller — a mucosal fold at the junction of the common canaliculus and lacrimal sac — prevents reflux from the sac back into the canaliculi during blinking. Injury to the canaliculus (e.g. lid laceration) requires careful repair with a monocanalicular or bicanalicular stent within 48 hours for best results.
Lacrimal Sac
The lacrimal sac lies in the lacrimal sac fossa, bounded anteriorly by the anterior lacrimal crest (maxillary bone) and posteriorly by the posterior lacrimal crest (lacrimal bone). The lacrimal bone is very thin and fragile — surgeons aim posteriorly during DCR (dacryocystorhinostomy) to avoid it.
The medial canthal tendon splits around the sac, with its anterior limb passing in front of it and the posterior limb behind. This relationship is critical during DCR — the anterior limb is cut to access the sac. Infection of the sac (dacryocystitis) presents as a red, tender swelling just below the medial canthus and may progress to abscess or fistula formation.
Nasolacrimal Duct
The nasolacrimal duct travels obliquely — slightly lateral and posterior — within the bony nasolacrimal canal. It opens approximately 2.5 cm posterior to the naris on the lateral nasal wall, beneath the inferior turbinate, covered by the valve of Hasner.
Congenital obstruction most commonly occurs at the valve of Hasner, which fails to canalize at birth in up to 6% of newborns. Most resolve spontaneously with massage within the first year; persistent obstruction is treated with probing and, if needed, intubation or DCR. Acquired obstruction in adults is most commonly idiopathic (primary acquired nasolacrimal duct obstruction — PANDO) and treated with DCR, which creates a new bony opening directly from the lacrimal sac to the nasal cavity, bypassing the duct entirely.
The Lacrimal Pump
Tear drainage is not passive — it depends on an active lacrimal pump mechanism driven by the orbicularis oculi muscle and the medial canthal tendon. With each blink:
- The pretarsal orbicularis contracts, compressing the canaliculi and pushing tears medially.
- The deep heads of the preseptal orbicularis (Horner’s muscle) contract around the lacrimal sac, creating negative pressure that draws tears in through the puncta.
- On lid opening, the sac expands, the valve of Rosenmüller opens, and tears drain into the nasolacrimal duct.
Pump failure — from orbicularis weakness (facial palsy), lid laxity, or punctal eversion — causes functional epiphora even when the drainage anatomy is intact. This distinction is important: a patient with tearing but patent irrigation has a pump problem, not a duct obstruction.
Clinical Relevance
Congenital NLDO
Valve of Hasner fails to open
Massage → probing → DCR
Acquired NLDO (PANDO)
Idiopathic fibrosis of duct mucosa
DCR (external or endoscopic)
Canalicular obstruction
Trauma, herpes, drug toxicity
Canaliculo-DCR, Jones tube
Dacryocystitis
Stasis → bacterial infection of sac
Antibiotics ± DCR
Functional epiphora
Pump failure, punctal malposition
Lid tightening, punctoplasty
Lacrimal gland tumor
Pleomorphic adenoma, lymphoma
Excision, biopsy, systemic treatment
Schedule a Consultation
Contact us to discuss tearing, blocked ducts, or lacrimal infections.