
Ptosis
Repair of drooping upper eyelids (ptosis) — both cosmetic and functional correction of levator muscle weakness.
What Is Ptosis

Ptosis (pronounced TOE-sis) is an abnormally low position of the upper eyelid. When the levator muscle — the primary eyelid elevator — or Müller’s muscle weakens, stretches, or detaches from the eyelid, the lid drops in front of the pupil. Ptosis may affect one eye or both and ranges from barely noticeable to severe enough to obstruct vision entirely.
- Ptosis is also called blepharoptosis
- It differs from dermatochalasis (excess upper eyelid skin) — though both conditions frequently coexist
- A drooping lid that crosses the pupil reduces the superior visual field, causes eyebrow strain and headaches, and in children can lead to amblyopia (“lazy eye”)
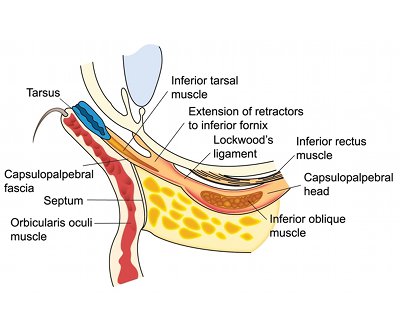
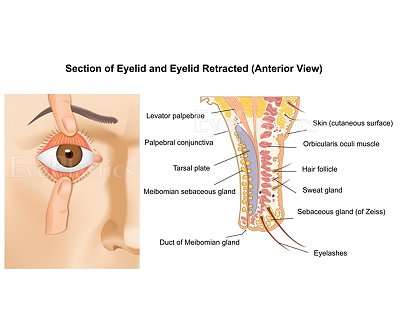
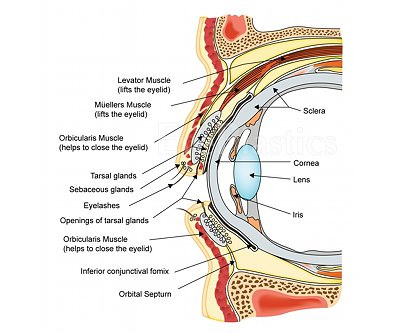
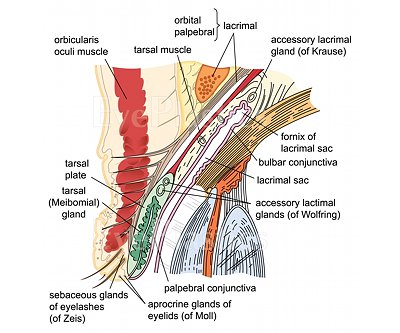
For a detailed guide to levator anatomy, Müller’s muscle, and the tarsal plate, see our dedicated Eyelid Anatomy page.
Evaluation of Ptosis
Careful measurement is the foundation of ptosis surgery planning. Dr. Brown records the following at every ptosis evaluation:
- Margin-reflex distance (MRD-1): the distance from the corneal light reflex to the upper lid margin in primary gaze. Normal ≈ 4–5 mm; ptosis is present when MRD-1 is < 2 mm
- Levator function: total lid excursion from full downgaze to full upgaze with the brow held still. Excellent ≥ 10 mm; fair 5–9 mm; poor ≤ 4 mm — this single measurement largely determines the surgical approach
- Lid crease height: the distance from the lash margin to the skin crease, which guides the incision level
- Phenylephrine test: a drop of 2.5% phenylephrine behind the upper lid stimulates Müller’s muscle; elevation of ≥ 1 mm predicts a favorable response to internal ptosis repair (MMCR)
Visual Field Impact
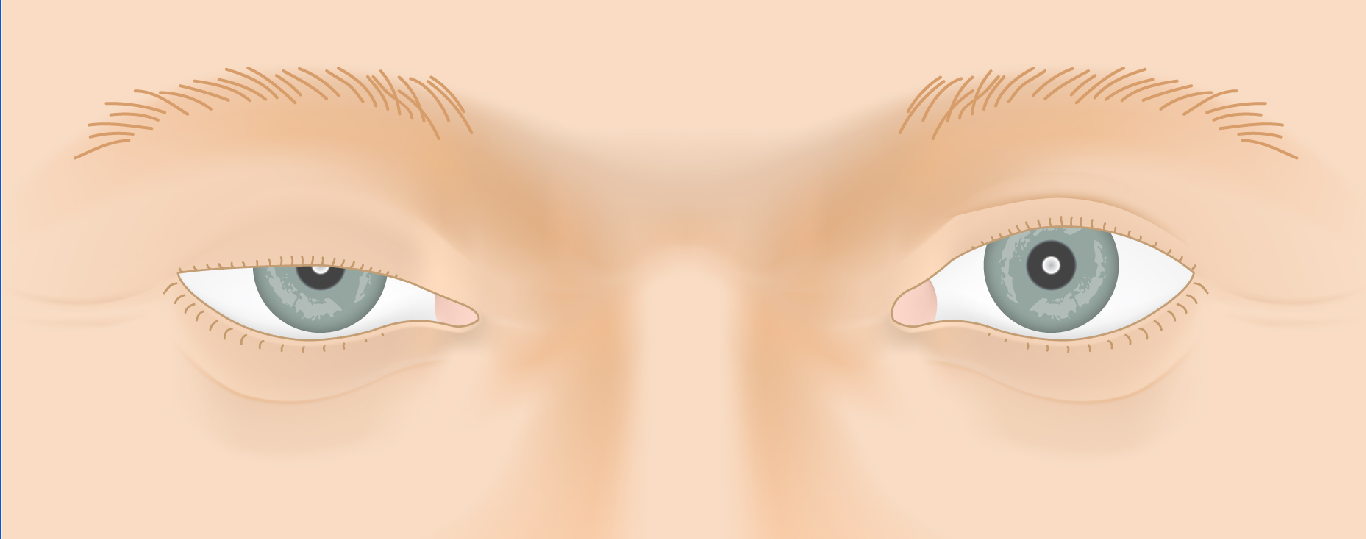
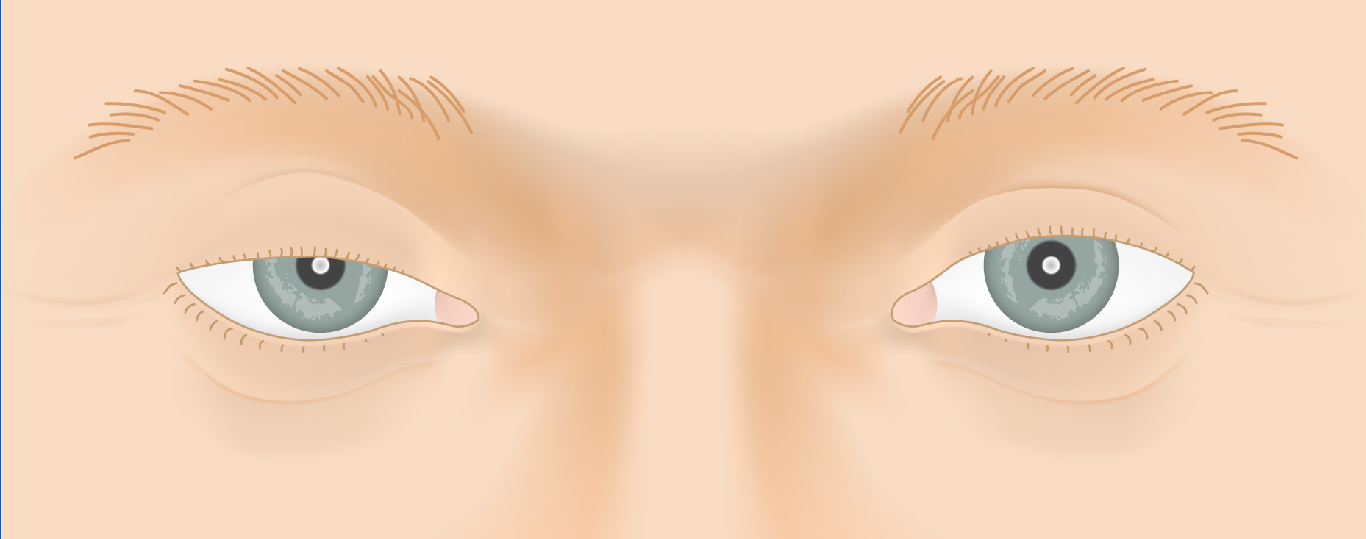
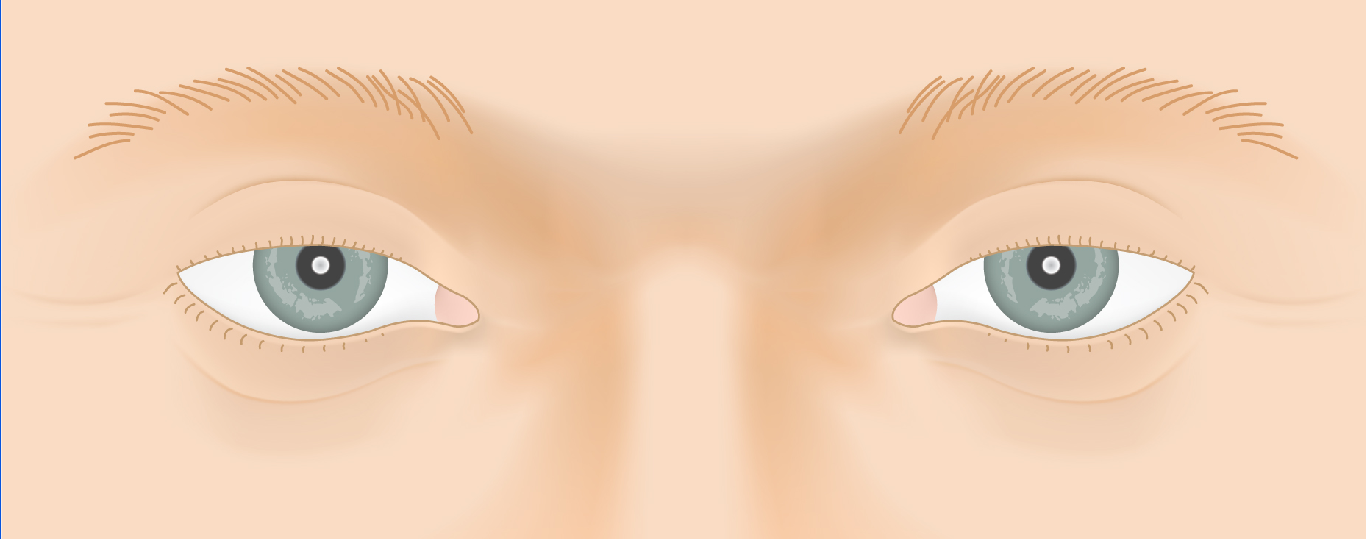
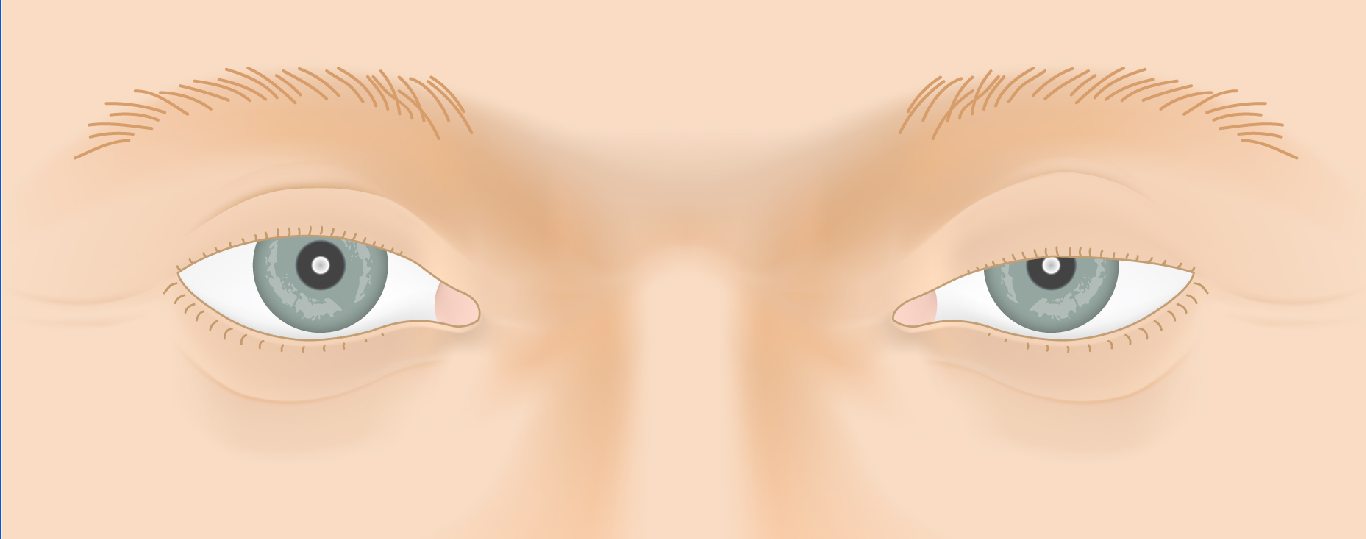
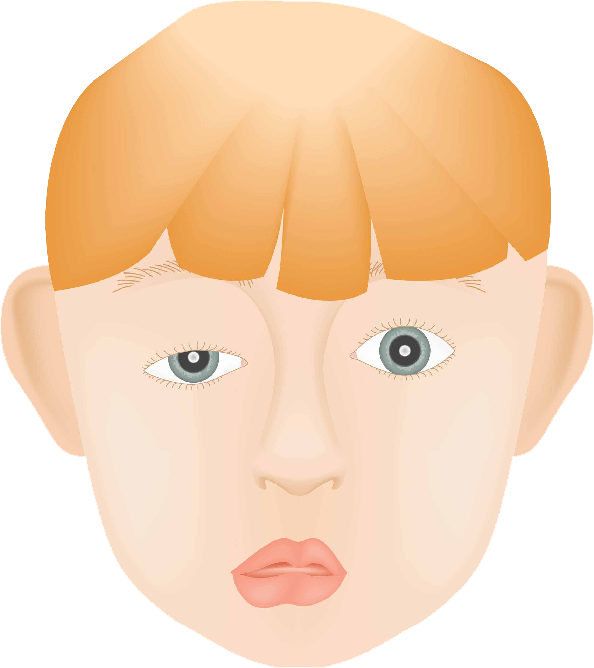
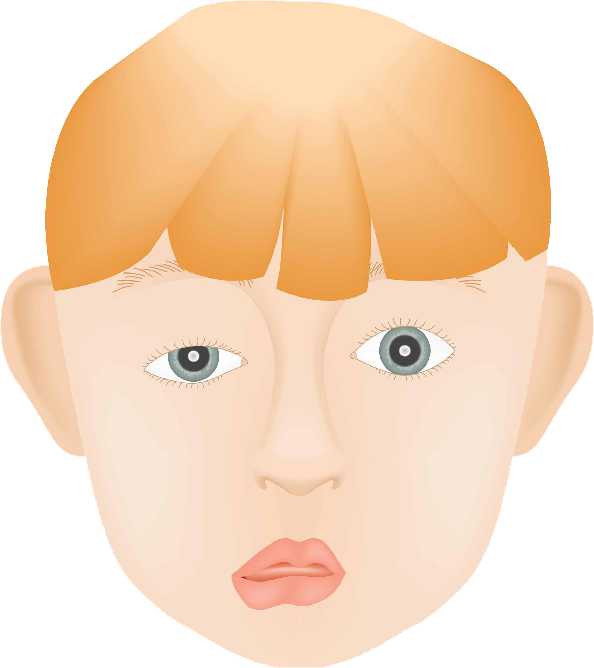
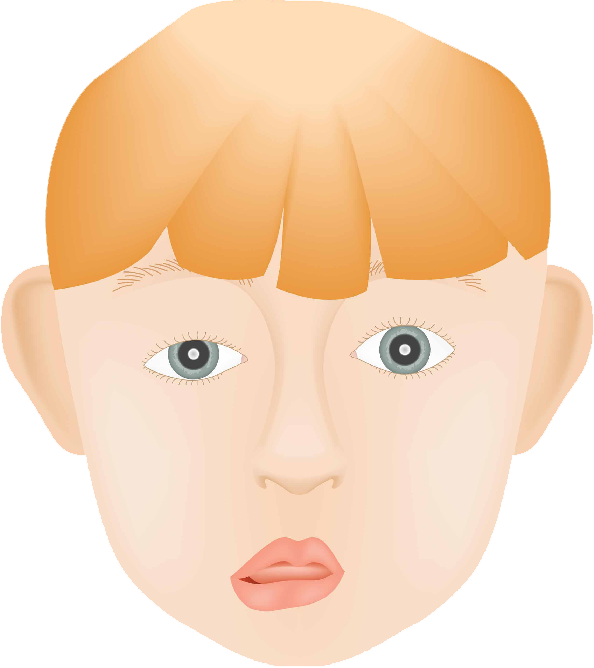
The animation below shows how a drooping upper eyelid progressively narrows the superior visual field.
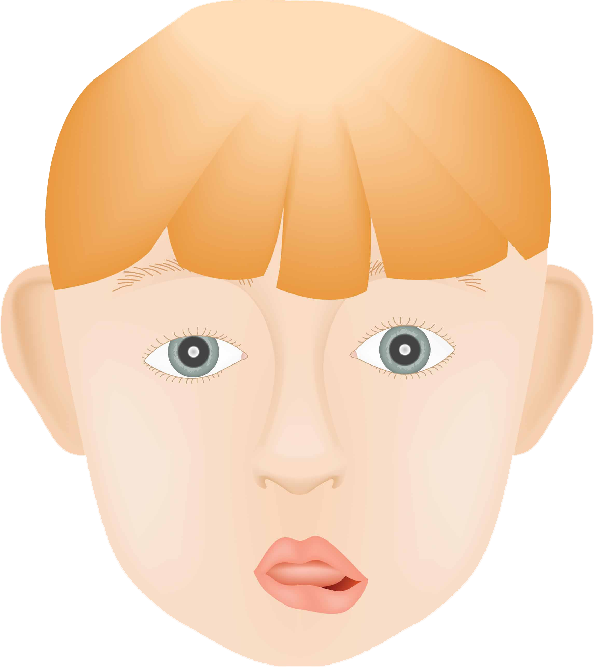
Visual Field Loss from Ptosis
Adjust the slider to visualize how a drooping upper eyelid progressively encroaches on the superior visual field.








Drag the slider to compare
Hering’s Law of Equal Innervation
When ptosis affects only one eye — or is much worse on one side — Hering’s law becomes critical to surgical planning. Both levators receive equal central drive from the brain. In unilateral ptosis, the brain increases drive to both sides to keep the ptotic lid open. If surgery elevates the ptotic lid, that extra drive drops — and the fellow lid may fall.
This “see-saw” effect means apparent unilateral ptosis can unmask bilateral ptosis after surgery on one side. The interactive animation below demonstrates this phenomenon.
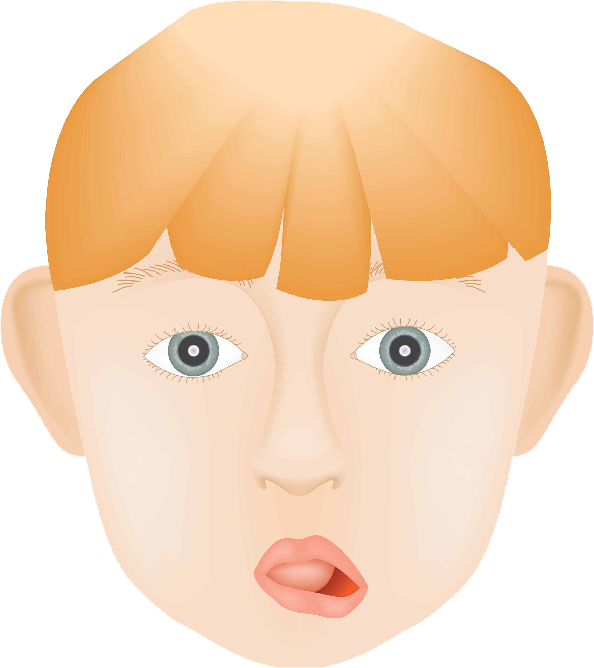
Ptosis — Hering's Law Visualization
Slide the control to see how ptosis in one eye affects the fellow eye according to Hering's Law of Equal Innervation.
Drag the slider to compare
Acquired Ptosis
Most adult ptosis is aponeurotic — the levator muscle is intact and still strong, but the fibrous aponeurosis (tendon) that transmits the muscle’s pull to the tarsus has stretched, thinned, or detached. The lid sits low not because of muscle weakness but because the mechanical connection is lost.
Common Causes
- Aging: the most common cause by far — the aponeurosis disinserts from the tarsus gradually over decades. Levator function typically remains excellent (≥ 10 mm)
- Long-term contact lens wear: repeated mechanical trauma from lens insertion and removal stretches the aponeurosis; a common cause in younger adults
- Prior intraocular surgery: lid speculum use during cataract surgery is a well-recognized precipitant
- Chronic eye rubbing or inflammation: repeated lid traction weakens the aponeurosis over time
- Myasthenia gravis: a neuromuscular disorder producing variable, fatigable ptosis that characteristically worsens as the day progresses — must be excluded before planning surgery
- Third nerve (CN III) palsy: causes complete ptosis with a dilated, unreactive pupil; the pupil-involving form is a neurological emergency requiring urgent imaging
Important: new-onset unilateral ptosis with a dilated, unreactive pupil requires same-day neurological evaluation to exclude cerebral aneurysm or transtentorial herniation.
Congenital Ptosis

Congenital ptosis results from a developmental dystrophy of the levator muscle itself — fibrosis replaces normal striated muscle fibers, leaving the muscle stiff and underpowered. Unlike aponeurotic ptosis, the levator function is poor from birth.
Clinical Features
- Ptosis ranges from mild (lid partially covers pupil) to severe (pupil completely occluded)
- Lid lag on downgaze is characteristic: because the fibrotic muscle cannot fully relax, the lid stays high when looking down — the opposite of acquired ptosis
- Associated findings: amblyopia in up to 20% of cases, strabismus in ≈ 31%, and astigmatism
- Children may tilt the head back into a “chin-up” posture to see under the drooping lid
When to Operate
Surgery is deferred until age 3–5 (“pre-school years”) when possible, so intraoperative cooperation is better and the child has had time for amblyopia treatment. However, when the lid occludes the visual axis and threatens vision development, correction must be performed earlier — even in infancy.
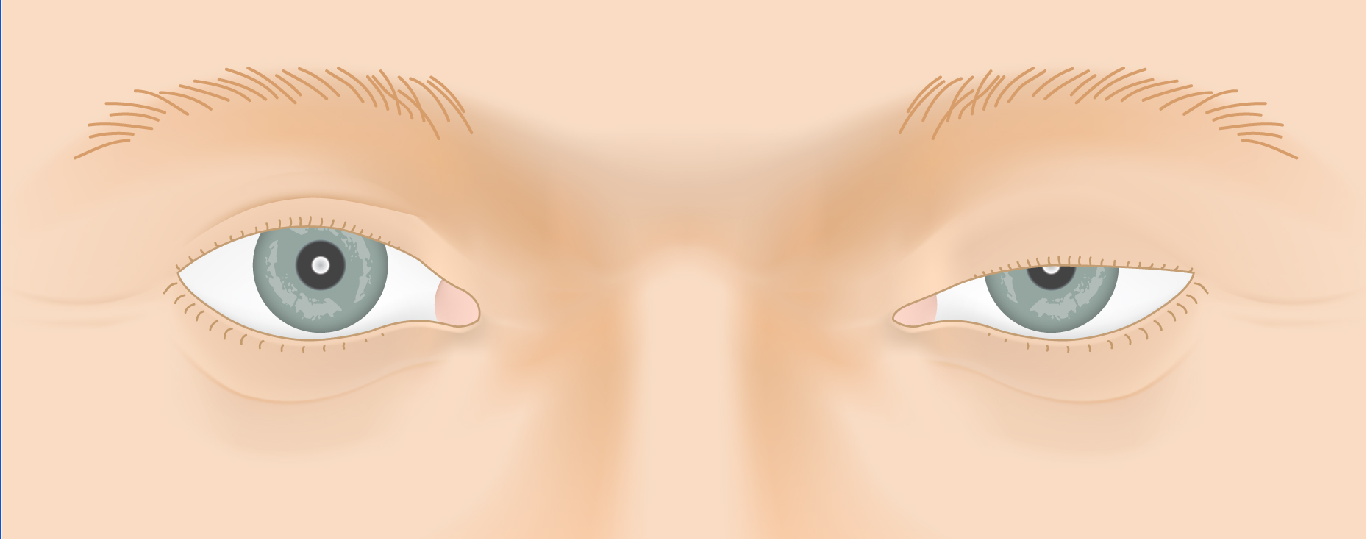
Horner’s Syndrome
Horner’s syndrome is caused by interruption of the sympathetic nerve pathway supplying the eye. Because sympathetic fibers innervate Müller’s muscle (the secondary upper lid elevator) and the inferior tarsal muscle, their loss produces a mild but distinctive ptosis of 1–2 mm.
Classic Triad
- Ptosis (upper lid, 1–2 mm) — Müller’s muscle denervation
- Inverse ptosis / lower lid elevation — inferior tarsal muscle denervation
- Miosis (small pupil) with dilation lag in dim light
Localizing the Lesion
The three-neuron sympathetic pathway is disrupted at different levels depending on the cause:
- First-order (central): hypothalamus to spinal cord — stroke, tumor, demyelination, syringomyelia
- Second-order (preganglionic): spinal cord to superior cervical ganglion — Pancoast tumor of the lung apex, carotid or subclavian artery pathology, cervical rib
- Third-order (postganglionic): superior cervical ganglion to orbit — carotid artery dissection, cavernous sinus mass, cluster headache
New-onset Horner’s syndrome requires urgent MRI/MRA to rule out carotid dissection or intracranial mass. In infants and children, Horner’s syndrome can cause heterochromia (lighter iris on the affected side) because sympathetic tone is needed for normal melanin development in the iris stroma.
Marcus Gunn Jaw Wink
Marcus Gunn jaw-wink ptosis is an example of synkinesis — an abnormal neural connection between two muscle groups that are normally unrelated. A branch of the trigeminal nerve (CN V, which supplies the pterygoid jaw muscles) misdirects into the branch of the oculomotor nerve (CN III) that lifts the upper eyelid. The result: the ptotic lid rises whenever the jaw opens or moves laterally.

Marcus Gunn Jaw Wink
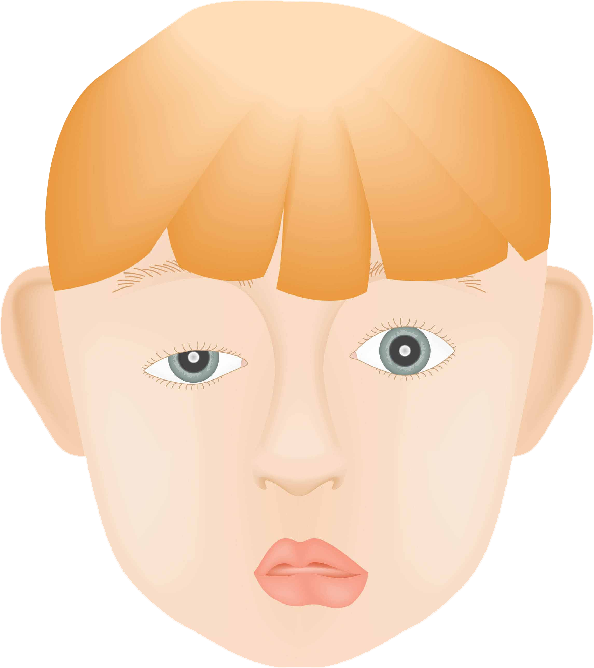

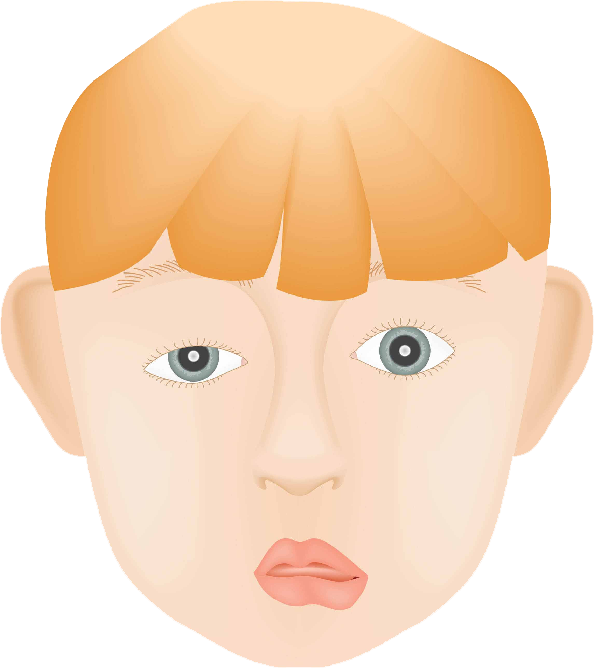
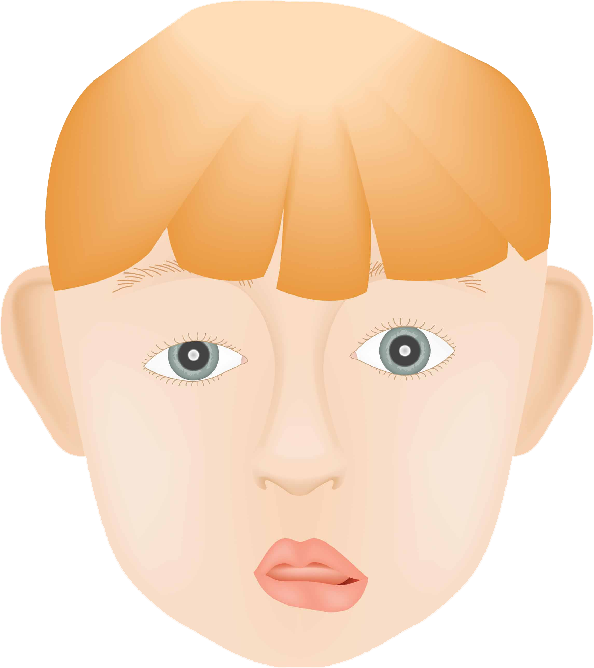
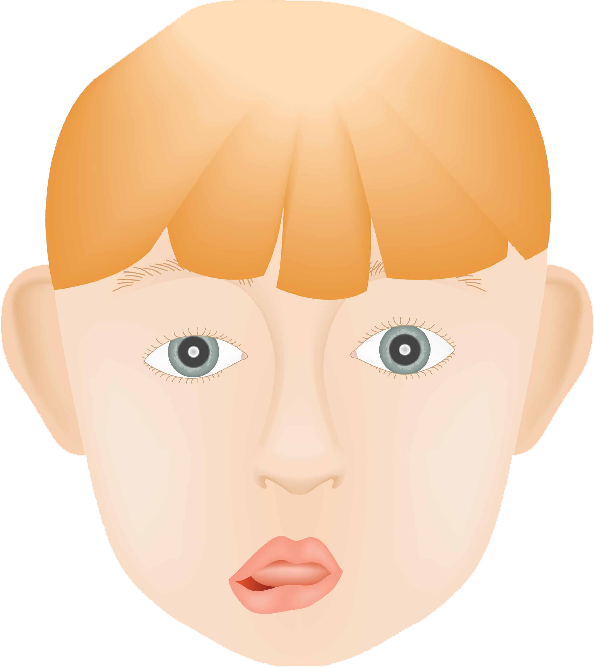

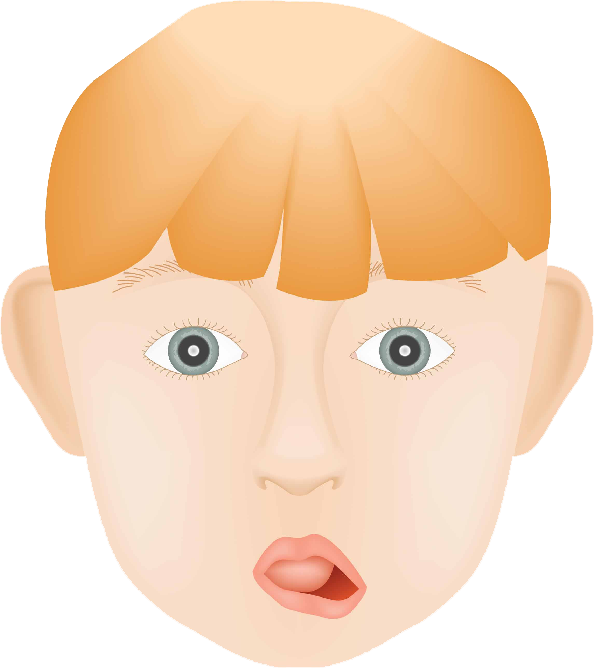


Slide the control to move the mouth.

Use the slider in the animation above to simulate the jaw-wink synkinesis — the eyelid rising as the jaw opens.
Key Features
- Occurs in 2–13% of patients with congenital ptosis
- Levator function is typically poor (≤ 4 mm)
- Does not improve spontaneously, though children learn to minimize visible jaw movement over time
- Associated strabismus in ≈ 60%, amblyopia in ≈ 35%
Treatment
The surgical approach is guided by the severity of both the ptosis and the jaw-wink:
- Mild jaw-wink with significant ptosis: unilateral frontalis sling may achieve acceptable symmetry
- Significant jaw-wink: bilateral levator muscle disinsertion followed by bilateral frontalis sling — this eliminates the synkinesis entirely and allows symmetrical correction
Ptosis vs. Blepharoplasty
Two distinct upper eyelid conditions are often confused. Understanding the difference determines which operation is appropriate — and whether insurance will cover it.
Ptosis
Drooping of the eyelid margin itself
- Eyelid margin sits too low across the pupil
- Caused by weak or detached levator / Müller’s muscle
- Little or no excess skin
- Surgery elevates the eyelid margin
- May be covered by insurance with visual field documentation
Dermatochalasis (Pseudoptosis)
Excess skin overhanging the lid
- Eyelid margin sits at normal height
- Overhanging skin hood blocks the superior field
- Repaired by blepharoplasty (skin removal)
- Can coexist with true ptosis
- Insurance-covered if skin obstructs the visual field
Both conditions can be present simultaneously. Ptosis repair and blepharoplasty are frequently combined in a single operation through the same eyelid crease incision.
Not sure which condition you have? Our Ptosis vs. Blepharoplasty Guide walks through the key differences with photographs.
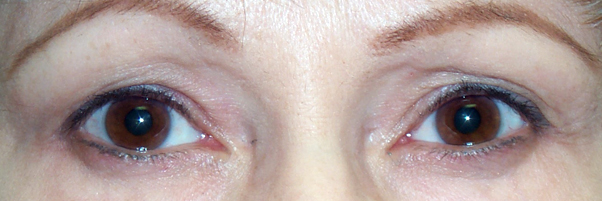
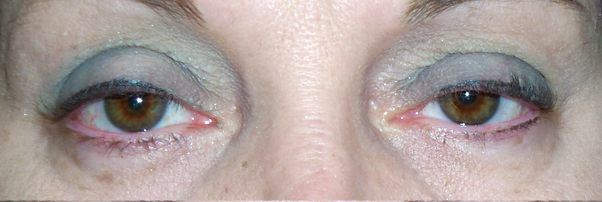
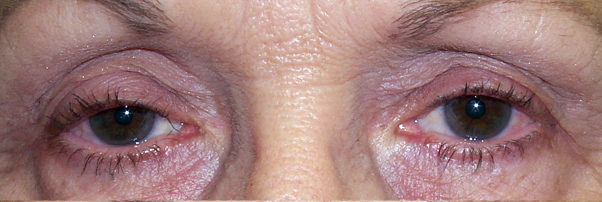
Ptosis + Upper Blepharoplasty Results
Drag the divider left or right to compare. Use arrow keys when focused.





Treatment of Ptosis
The choice of operation depends on three factors: the degree of ptosis, the remaining levator function, and the phenylephrine test result. Dr. Brown reviews all options with you at consultation and tailors the approach to your anatomy and goals.
Müller Muscle–Conjunctival Resection (MMCR — Internal Approach)
- Incision made through the inner conjunctival surface of the lid — no external scar
- Best candidates: good levator function (≥ 10 mm) and a positive phenylephrine test
- The amount of Müller muscle and conjunctiva resected is determined by a formula based on the phenylephrine response
- Patient is under general or IV sedation (no intraoperative adjustment needed)
- Can be combined with cosmetic upper blepharoplasty
Levator Advancement (External Approach)
- Incision placed within the upper lid crease — scar is hidden in the natural skin fold
- The aponeurosis is reattached or tightened to the tarsus under direct vision
- Patient is awake during the key adjustment step so lid height and contour can be refined in real time
- Preferred for aponeurotic ptosis with moderate-to-good levator function
- Can be combined with cosmetic upper blepharoplasty through the same incision
Frontalis Sling
- The eyelid is suspended directly from the frontalis (forehead) muscle using a sling material
- Required for severe ptosis with poor levator function (≤ 4 mm) — the typical situation in congenital ptosis and Marcus Gunn jaw wink
- Sling materials include autogenous fascia lata (harvested from the thigh), silicone rod, or Gore-Tex
- The patient opens their eye by raising their brow, not by contracting the levator
- Lagophthalmos (incomplete lid closure on downgaze and during sleep) is expected; lubricating eye drops are needed long-term
- Performed under general anesthesia; lid height is determined by a surgical formula
Ptosis Surgical Repair — Interactive Animation
Explore eyelid anatomy and the three main ptosis repair techniques: Internal, External, and Frontalis Sling.
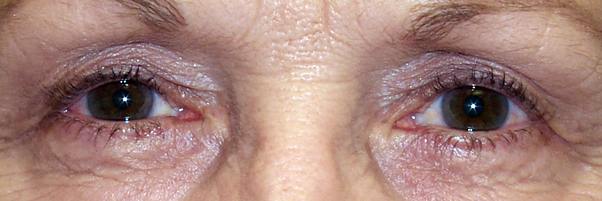
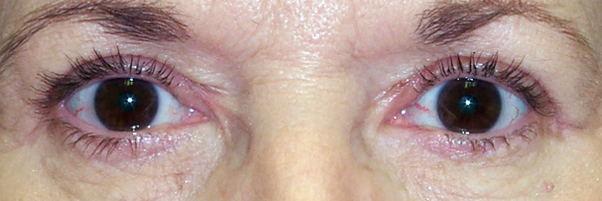
Ptosis Surgery Results
Drag the divider left or right to compare. Use arrow keys when focused.


Upneeq®
Upneeq® (oxymetazoline hydrochloride ophthalmic solution 0.1%) is the first and only FDA-approved prescription eye drop for acquired low-lying eyelids in adults. It is a non-surgical option for patients with mild ptosis.
How It Works
Oxymetazoline is an α-adrenergic agonist that selectively stimulates Müller’s muscle, lifting the upper eyelid by approximately 1 mm within 5 minutes of instillation. The effect lasts up to 8 hours.
Key Facts
- Once-daily drop applied to each ptotic eye
- Single-use, preservative-free container; discard after each dose
- Contact lenses must be removed before instillation; may be reinserted 15 minutes later
- Average eyelid lift is ≈ 1 mm — meaningful for mild ptosis; not sufficient for moderate or severe ptosis
- Clinical trials showed statistically significant improvement in superior visual field at 2 and 6 hours post-dose
Who Is a Candidate
- Adults with mild acquired aponeurotic ptosis who prefer a non-surgical option
- Patients who show lid elevation on the phenylephrine test
- Patients who are not yet surgical candidates due to other health conditions
Precautions
- Use with caution in patients with cardiovascular disease, uncontrolled hypertension or hypotension, or orthostatic hypotension — alpha-agonists affect vascular tone
- May increase the risk of angle closure glaucoma in patients with untreated narrow-angle glaucoma
- New ptosis with a variable or fatigable pattern (suggesting Myasthenia Gravis), or with a dilated unreactive pupil, requires specialist evaluation before Upneeq is prescribed
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.