Thyroid Eye Disease
Comprehensive treatment of Thyroid Eye Disease (TED / Graves' ophthalmopathy) — Dr. Brown has managed TED patients for over 20 years.
What Is Thyroid Eye Disease

Thyroid Eye Disease (TED) — also called Graves’ ophthalmopathy or thyroid-associated orbitopathy — is an autoimmune inflammatory condition of the orbit that occurs when the immune system attacks the tissues behind the eyes. It is most commonly, though not exclusively, associated with Graves’ disease (autoimmune hyperthyroidism).
- TED affects up to 50% of patients with Graves’ disease to some degree; clinically significant disease occurs in 25–30%
- Severe, vision-threatening disease occurs in 3–5% of cases
- Female-to-male ratio is approximately 5:1; peak incidence in the 4th and 5th decades
- Smoking is the single most important modifiable risk factor — it significantly worsens disease activity and reduces response to treatment
- TED can be present even when thyroid hormone levels are normal (“euthyroid Graves’ disease”)
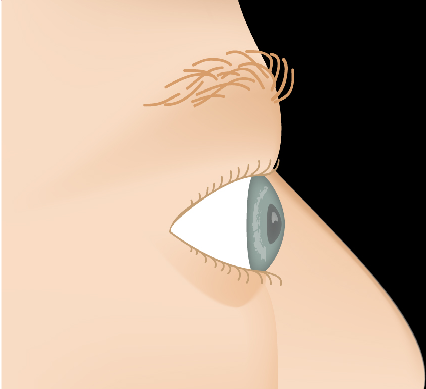
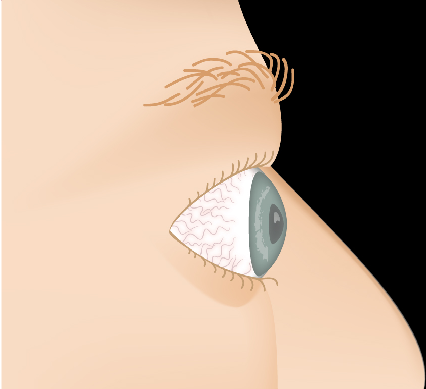
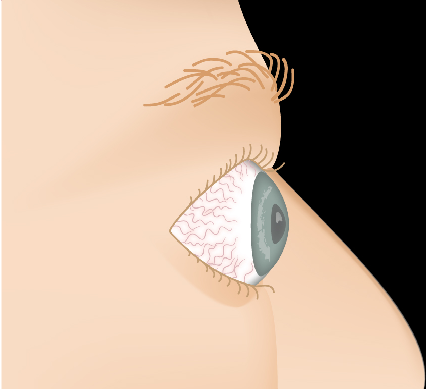
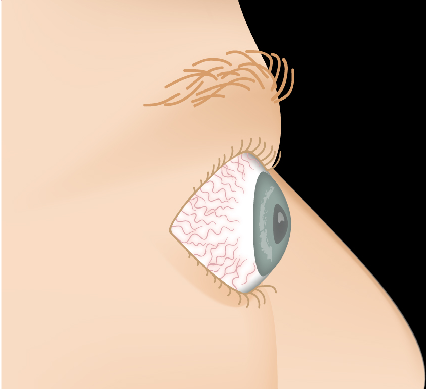
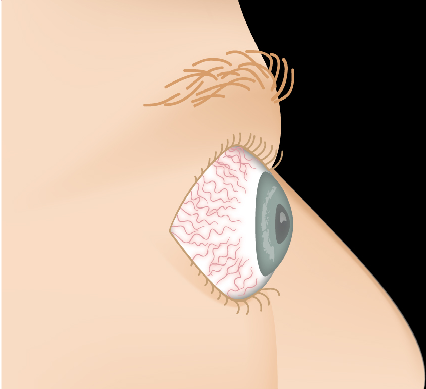
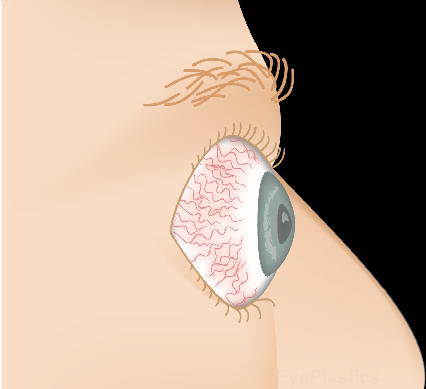
Thyroid Eye Disease — Disease Progression
Slide the control to visualize the progression from a healthy appearance to advanced Graves' ophthalmopathy (TED).
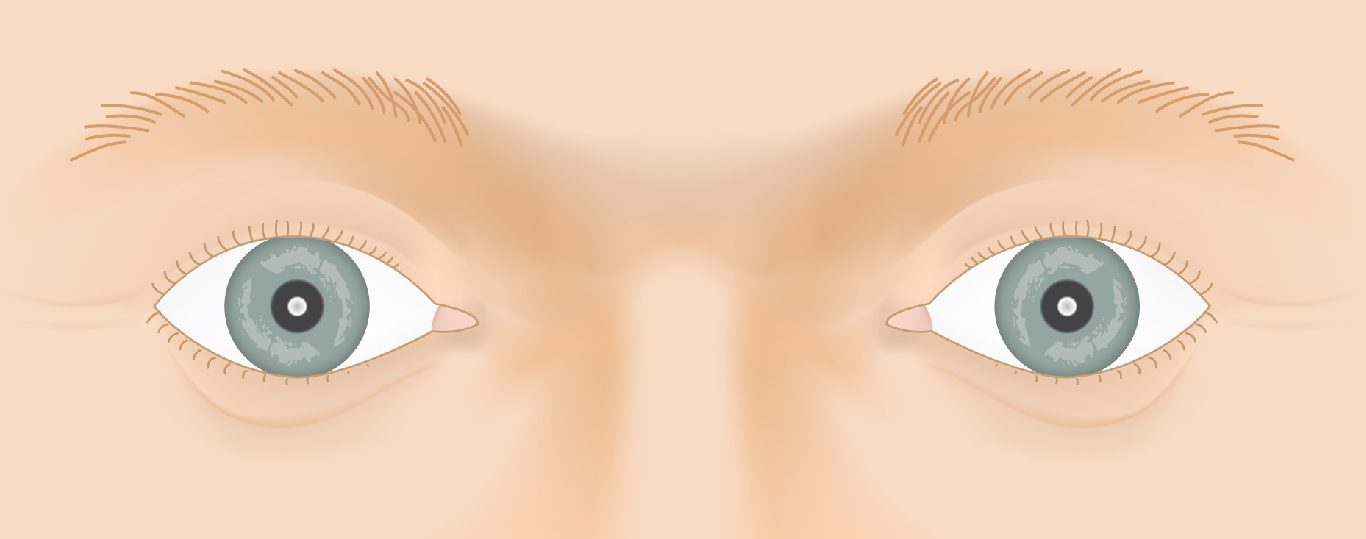
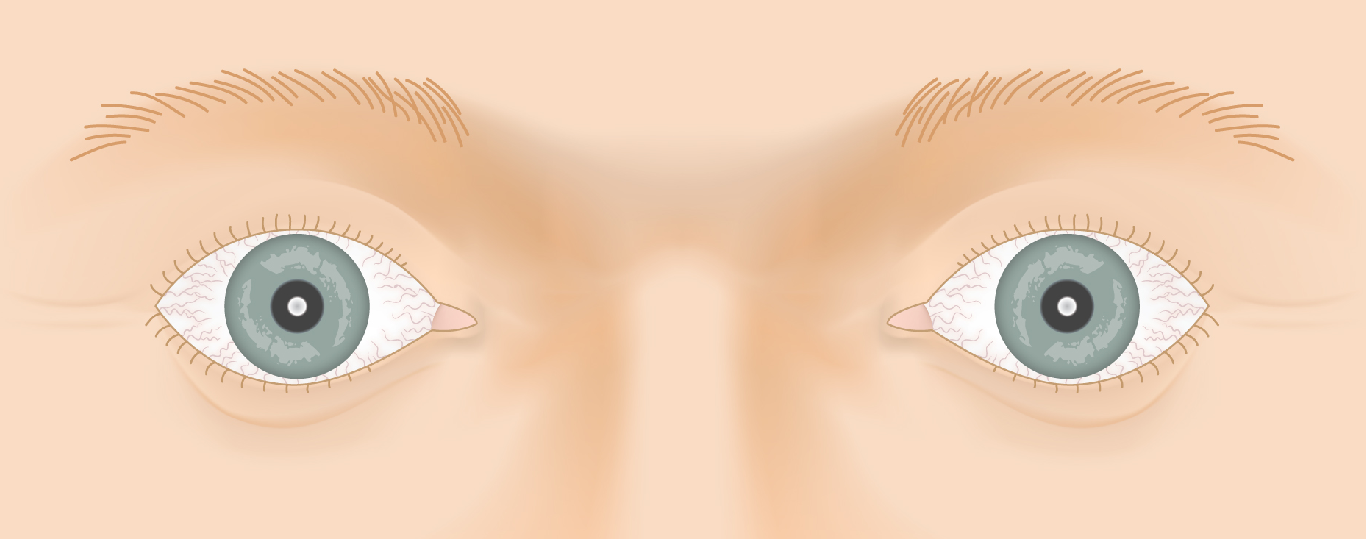
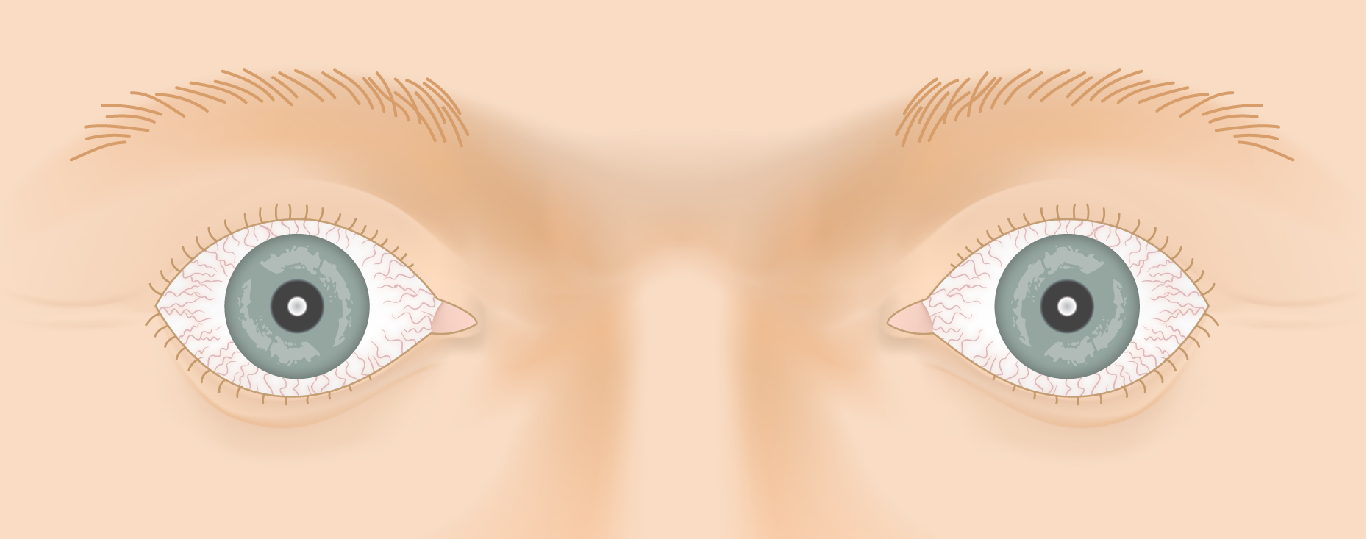
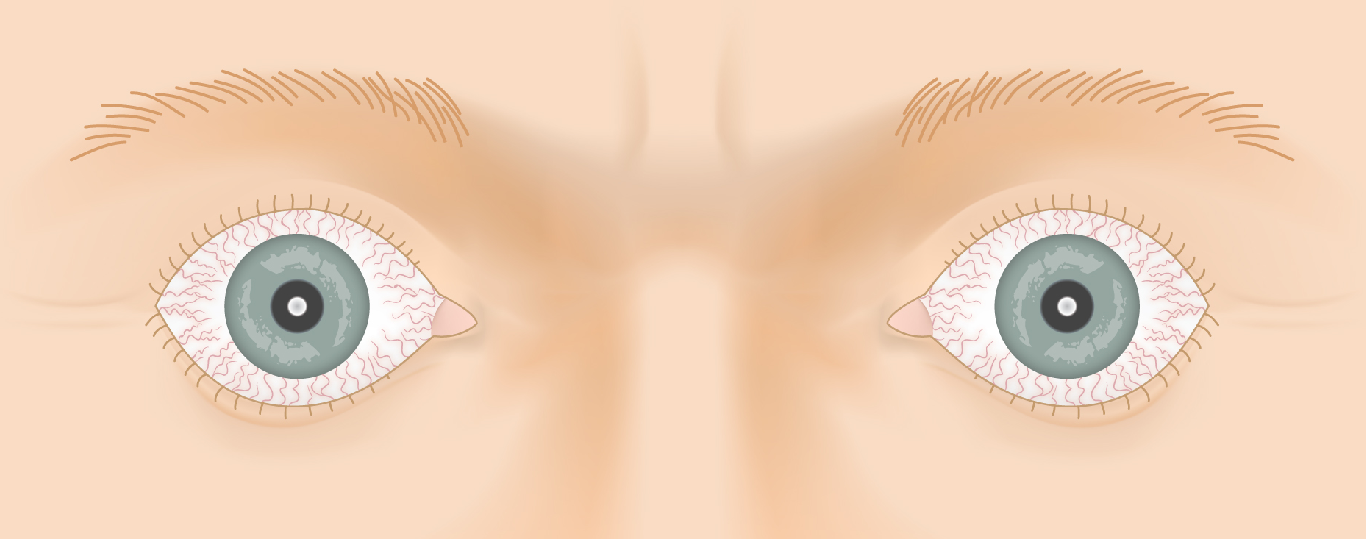
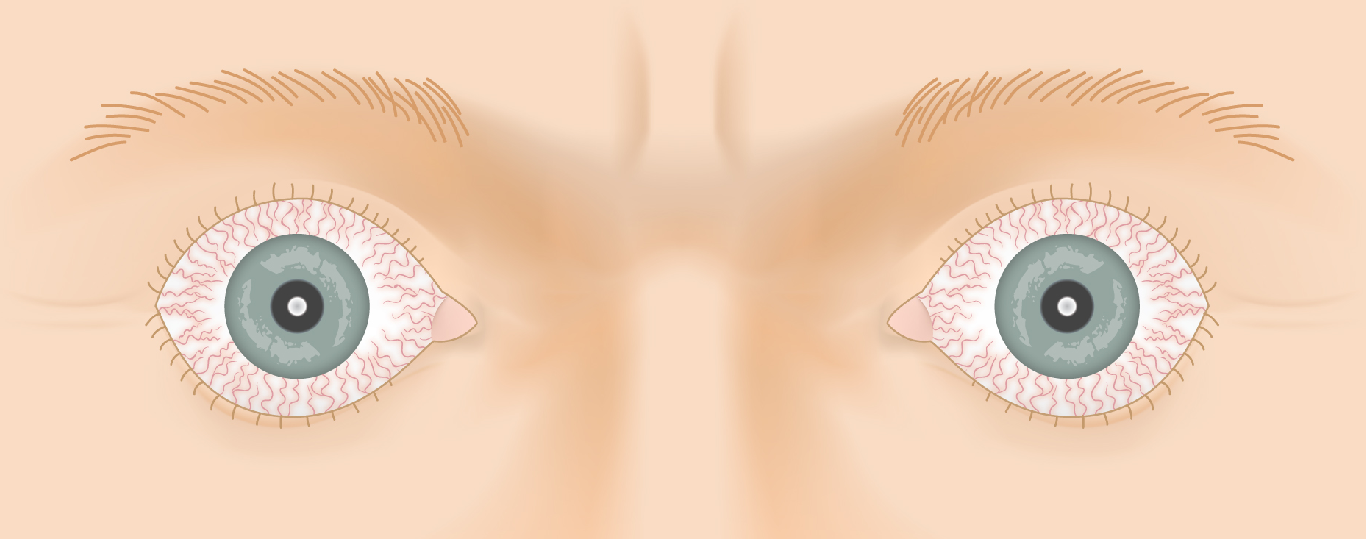
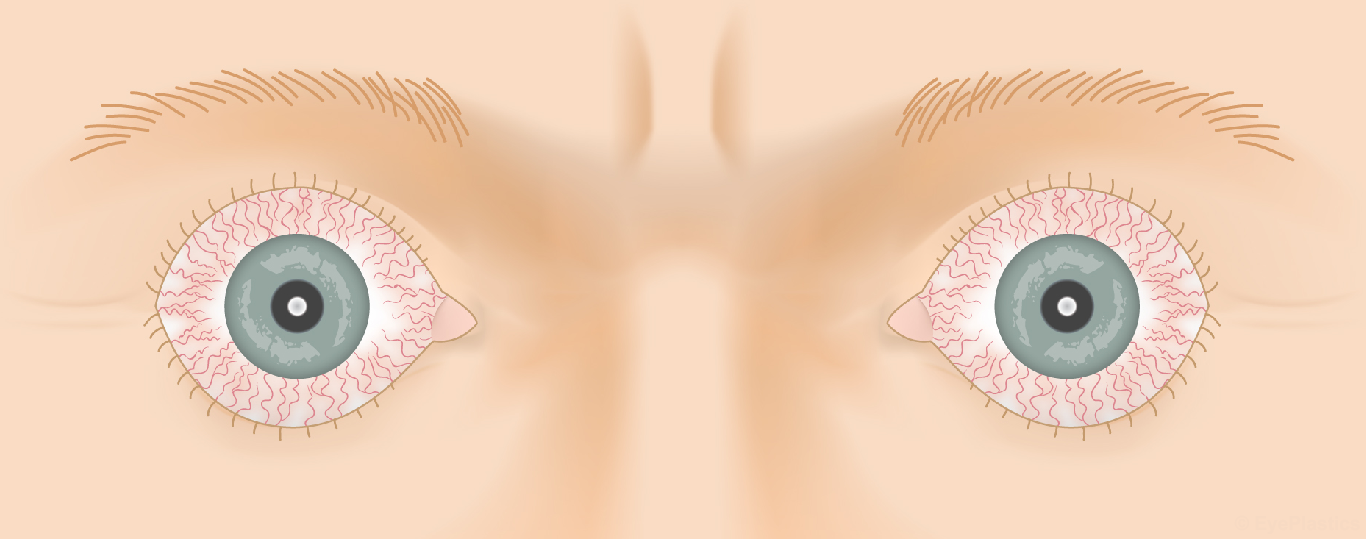
Drag the slider to compare
Graves’ Disease & How It Affects the Eye
Graves’ disease is an autoimmune disorder in which the body produces antibodies against the thyroid-stimulating hormone receptor (TSH-R). These anti-TSH-R antibodies (also called TSHR-Ab, TRAb, or TSI) do two things simultaneously:
- In the thyroid: they stimulate the gland to overproduce thyroid hormone, causing hyperthyroidism (rapid heart rate, weight loss, tremor, heat intolerance)
- In the orbit: the same TSH-R is expressed on orbital fibroblasts — the antibodies activate these cells, triggering inflammation, fibrosis, and expansion of extraocular muscles and orbital fat
The result is a crowded, inflamed orbit that pushes the eye forward (proptosis), restricts eye movement, and exposes the cornea. Because the thyroid and orbital disease share the same autoimmune trigger, treatment of the thyroid does not always resolve the eye disease — and radioactive iodine treatment can sometimes worsen TED.
Thyroid Function Tests in TED
At your evaluation, thyroid function is assessed with:
- TSH — low in hyperthyroidism; normal or elevated in hypothyroidism
- Free T4 and Free T3 — elevated in Graves’ hyperthyroidism
- TRAb / TSI — Thyroid receptor antibodies; typically elevated in active TED even when thyroid levels are controlled. These antibodies also predict disease severity and response to Tepezza
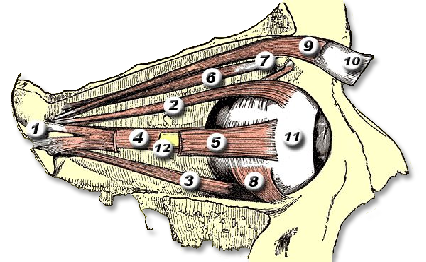
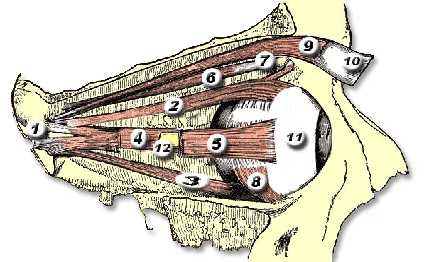
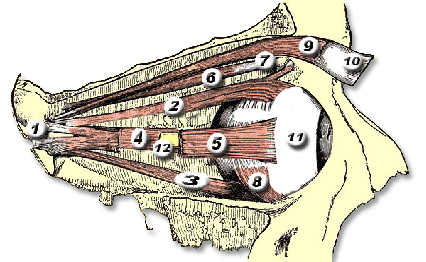
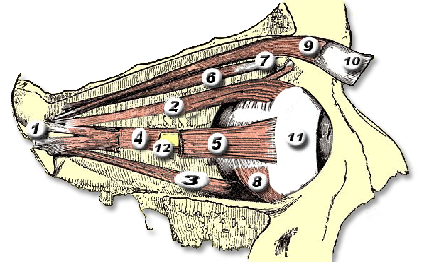
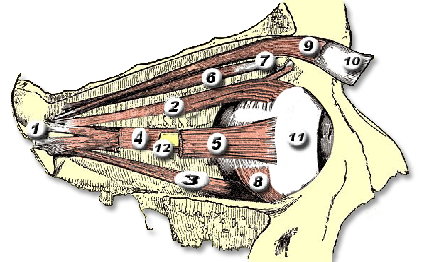
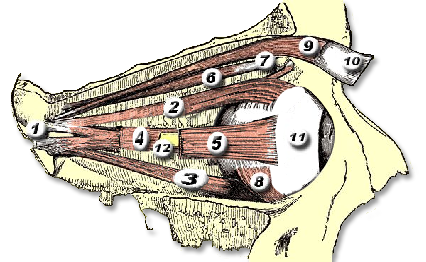
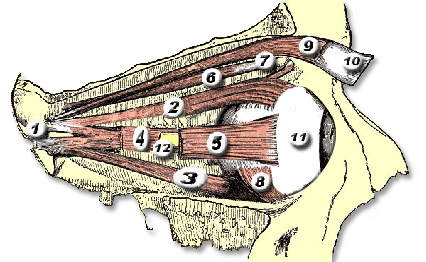
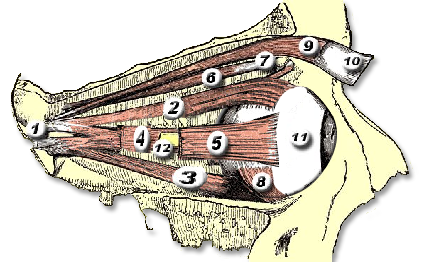
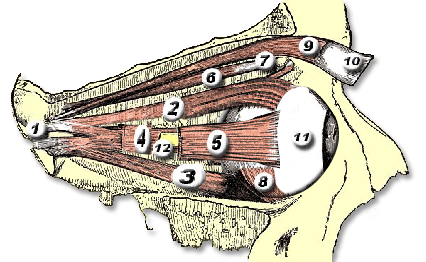
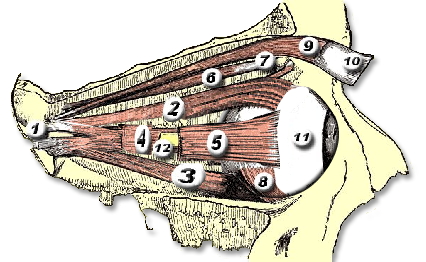
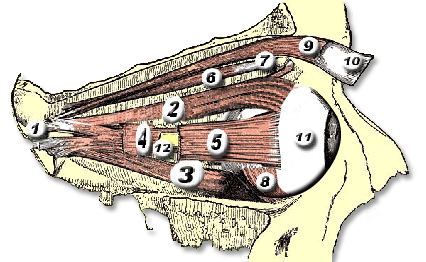
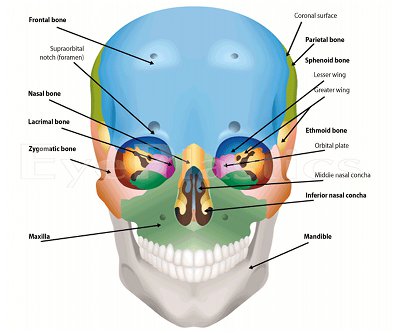
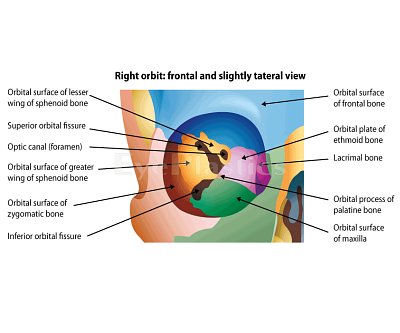
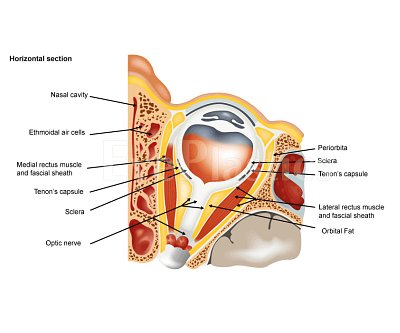
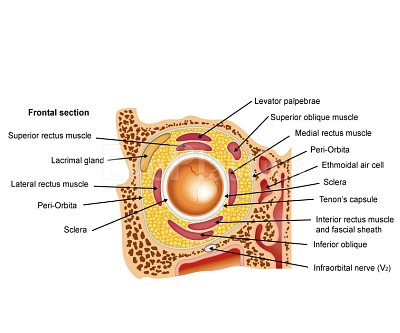
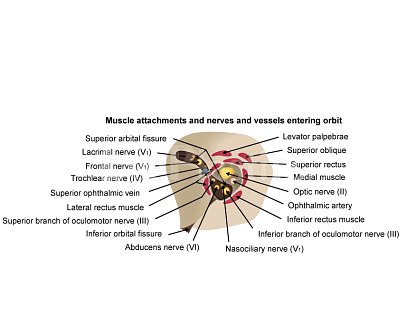
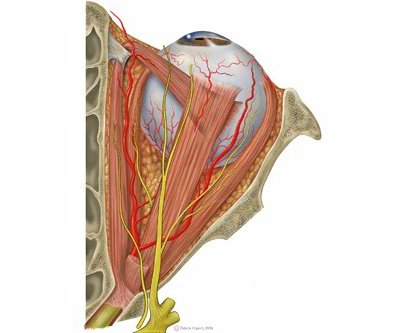
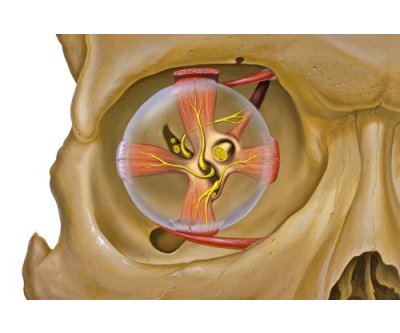
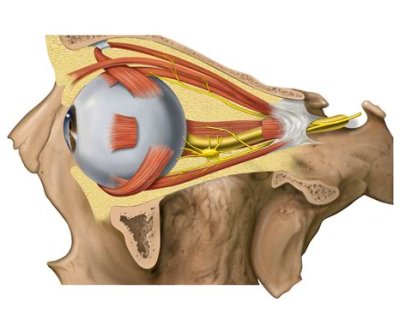
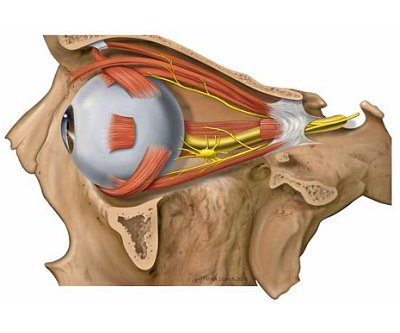
Orbital & Muscle Anatomy

In TED, the extraocular muscles become infiltrated with inflammatory cells, expand due to glycosaminoglycan deposition, and eventually fibrosis. The inferior and medial rectus muscles are most consistently affected, producing the characteristic upward and outward gaze restrictions and diplopia.
| Muscle | Primary Function | TED Involvement |
|---|---|---|
| Inferior rectus | Depression (downgaze) | Most commonly enlarged — causes hypotropia and limited upgaze; compresses optic nerve at apex |
| Medial rectus | Adduction | Second most affected — causes esotropia and limited abduction; diplopia on lateral gaze |
| Superior rectus / levator | Elevation / lid opening | Enlargement restricts downgaze; levator fibrosis and sympathetic Müller muscle stimulation cause lid retraction |
| Lateral rectus | Abduction | Less commonly enlarged |
| Superior oblique | Intorsion / depression | Rarely affected |
For detailed orbital bone and muscle anatomy, see our Orbital Anatomy page.
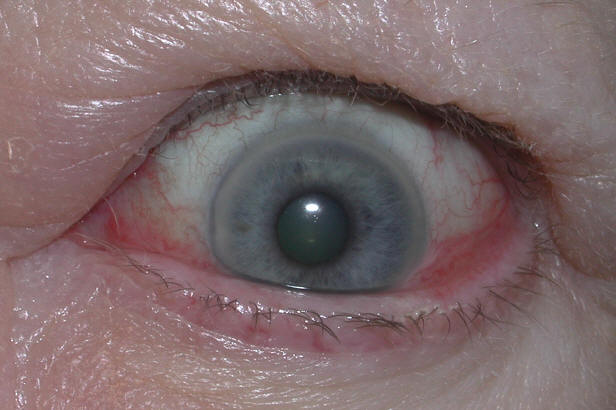
Eye Signs of Thyroid Eye Disease

The hallmark findings of TED include proptosis, lid retraction, restricted eye movement, and periorbital swelling. The combination of these features gives the characteristic “staring” or “startled” appearance.
Clinical Findings
- Proptosis (exophthalmos): Forward displacement of the globe due to expanded orbital volume. Hertel exophthalmometry >21 mm or >2 mm asymmetry is significant. Bilateral proptosis is the most common cause of proptosis in adults
- Eyelid retraction: Upper lid scleral show (limbus to upper lid margin >2 mm) and lower lid scleral show below the limbus. Both sympathetic over-stimulation and levator fibrosis contribute
- Restrictive strabismus: Tight, fibrotic extraocular muscles restrict movement and cause diplopia, most commonly on upgaze (inferior rectus) and lateral gaze (medial rectus)
- Periorbital edema and chemosis: Inflammatory swelling of eyelids, conjunctiva, and caruncle
- Corneal exposure keratopathy: Incomplete eyelid closure and reduced blink rate from proptosis and lid retraction expose the cornea — causing dryness, pain, and risk of corneal ulceration
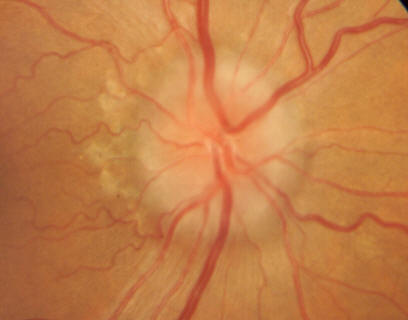
- Compressive optic neuropathy (CON): The most vision-threatening complication — enlarged muscles at the orbital apex compress the optic nerve. Presents with decreased visual acuity, color desaturation, and relative afferent pupillary defect. Requires urgent treatment
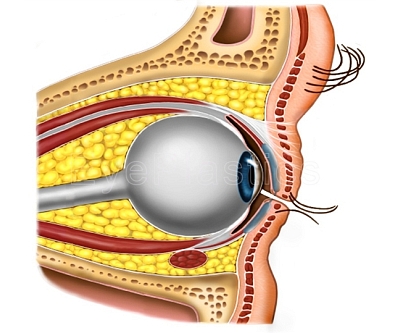
Proptosis — Orbital Changes
Interactive visualization showing orbital muscle changes and progressive proptosis associated with Thyroid Eye Disease.
Drag the slider to compare
Radiological Findings


CT of the orbits characteristically demonstrates enlarged extraocular muscles (particularly inferior and medial rectus) with sparing of the tendinous insertions — a key feature distinguishing TED from orbital myositis, where the tendon is involved. The apex-to-equator ratio of enlargement predicts risk of optic neuropathy.
Disease Activity & Severity
TED has two distinct phases: an active (inflammatory) phase of variable duration (typically 6–24 months) followed by an inactive (fibrotic) phase. Timing of treatment is critical — most medical therapies work only during the active phase.
Clinical Activity Score (CAS)
The CAS assigns one point for each of the following signs of active inflammation:
- Spontaneous orbital pain
- Pain on eye movement
- Eyelid erythema
- Conjunctival injection
- Chemosis
- Swelling of the caruncle or plica
- Eyelid edema
A CAS ≥ 3/7 indicates active disease. Active disease responds to immunosuppression (steroids, Tepezza); inactive disease does not — surgical rehabilitation is the appropriate approach for stable inactive TED.
Severity Classification
Mild TED
- Minimal impact on quality of life
- Lid retraction < 2 mm
- Proptosis < 3 mm above normal
- Mild corneal exposure
- Transient or no diplopia
- Managed conservatively; observation is appropriate
Moderate-to-Severe TED
- Significant impact on daily life
- Lid retraction ≥ 2 mm
- Proptosis ≥ 3 mm above normal
- Intermittent or constant diplopia
- Corneal exposure requiring treatment
- Active disease requires Tepezza or IV steroids
Sight-threatening TED: Compressive optic neuropathy or severe corneal exposure requires urgent treatment — urgent high-dose IV corticosteroids and/or orbital decompression surgery regardless of disease phase.
Conservative Management
- Preservative-free lubricating eye drops (frequently) and gel or ointment at night
- Selenium supplementation 200 μg/day for 6 months — shown to slow progression in mild active TED
- Taping eyelids closed at night for lagophthalmos
- Elevated head of bed to reduce morning periorbital edema
- Prism glasses for diplopia
- Smoking cessation — the single most impactful intervention a patient can make
Strabismus & Double Vision

Diplopia (double vision) in TED results from restrictive strabismus — the inflamed, fibrotic extraocular muscles tether the eye and prevent full movement, causing misalignment. Unlike paralytic strabismus, TED strabismus features a positive forced duction test (the eye cannot be passively moved through full range).
Patterns
- Inferior rectus restriction (most common): hypotropia (eye deviated down) with limited upgaze. Patient cannot look up and sees double in primary or downgaze positions
- Medial rectus restriction: esotropia (eye deviated in) with limited abduction. Double vision on lateral gaze
- Restrictive strabismus is variable in active disease — surgery is deferred until disease is stable (≥ 6 months without change)
Treatment
- Prism glasses: fresnel prisms adhered to spectacle lenses can neutralize small deviations; useful during active disease while waiting for stability
- Strabismus surgery: recession (lengthening) of the tight, overacting muscle — the muscle is detached from the globe and reattached further back. Goals are single vision in primary gaze and reading position. More than one procedure is sometimes needed
- Strabismus surgery is performed before eyelid surgery in the sequence: orbital decompression → strabismus → eyelid
Eyelid Retraction
Eyelid retraction is among the most common and distressing features of TED. The upper lid normally covers 1–2 mm of the superior limbus; in TED it may sit above the limbus entirely, exposing the sclera and giving the characteristic staring appearance.
Causes of Upper Lid Retraction in TED
- Overactive sympathetic tone (Müller muscle stimulation from hyperthyroidism) — often partially reversible with thyroid control
- Levator muscle fibrosis — the levator becomes adherent to surrounding tissues; responds only to surgery
- Inferior rectus restriction with compensatory upgaze effort — increased levator drive to elevate the globe worsens lid retraction; strabismus surgery may reduce this component
Consequences
- Corneal exposure: dryness, punctate keratitis, corneal ulceration in severe cases
- Lagophthalmos (inability to close lids fully during sleep)
- Significant cosmetic distress
Surgical Correction
Eyelid surgery is the last step in the sequential rehabilitation of TED (after decompression and strabismus if needed), performed once disease is stable for ≥ 6 months.
- Upper lid lowering: Müller muscle recession (müllerectomy), levator recession, or eyelid spacer graft (using donor sclera, hard palate mucosa, or synthetic spacer) to lengthen the posterior lamella. Can lower the upper lid by 2–8 mm depending on technique
- Lower lid raising: Recession of the lower lid retractors with or without a spacer graft. Lateral tarsal strip canthoplasty to improve lower lid position and support
- Tarsorrhaphy: Partial closure of the lateral eyelids as a temporary or permanent measure for severe corneal exposure when definitive surgery is not yet possible
Orbital Decompression
Orbital Decompression — Surgical Animation
Explore orbital anatomy, clinical findings, and the medial wall, lateral wall, and floor decompression surgical techniques.
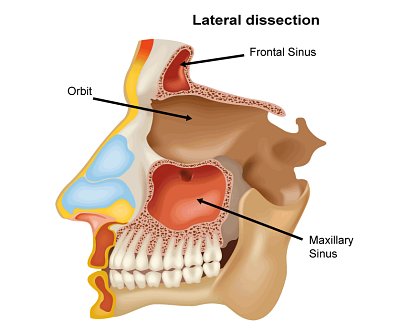
Orbital decompression creates additional volume within the orbit by removing one or more orbital walls, allowing the expanded orbital contents to bulge into the adjacent sinuses. This reduces proptosis, relieves corneal exposure, and — crucially — decompresses the optic nerve when vision is threatened.
Indications
- Compressive optic neuropathy — urgent or emergency decompression to prevent irreversible vision loss
- Severe proptosis with corneal exposure not controlled by medical means
- Cosmetic improvement of disfiguring proptosis in inactive disease
- Preparation for strabismus surgery (changing orbital volume may affect alignment)
Surgical Approach
Dr. Brown tailors the approach to each patient’s CT anatomy, severity, and goals:
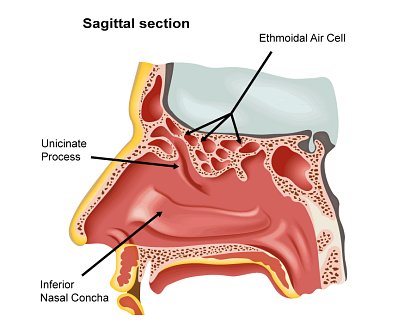
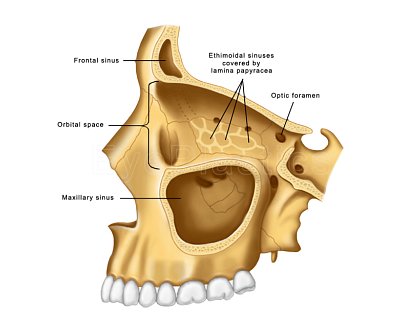
- Medial wall decompression: Removes the lamina papyracea (thin paper bone between orbit and ethmoid sinuses). Excellent for optic nerve decompression; 2–4 mm proptosis reduction per wall
- Orbital floor decompression: Opens the floor into the maxillary sinus; additional 2–4 mm reduction
- Lateral wall decompression: Opens into the temporal fossa; significant volume; lower risk of new diplopia compared to medial/floor
- 3-wall balanced decompression: Used for severe proptosis; may combine medial, floor, and lateral walls for maximum effect (6–10 mm proptosis reduction)
Risks & Recovery
- New or worsened diplopia is the most common significant complication — medial wall decompression carries the highest risk; balanced decompression with lateral wall reduces this
- Infraorbital numbness (cheek, upper lip) — usually temporary, lasting weeks to months
- CSF leak (rare) when decompressing near the skull base
- Vision improvement is expected when surgery is performed urgently for optic neuropathy; elective cosmetic decompression carries a very low risk of vision loss
Tepezza®
Tepezza® (teprotumumab-trbw) is the first FDA-approved treatment for Thyroid Eye Disease (approved 2020). It is a fully human monoclonal antibody that blocks the insulin-like growth factor 1 receptor (IGF-1R) — a key driver of the orbital inflammation and fibrosis underlying TED.
How It Works
In Graves’ disease, TSH-R antibodies activate orbital fibroblasts in part through cross-activation of the IGF-1R pathway. Tepezza blocks this receptor, dramatically reducing orbital inflammation, proptosis, and diplopia. It works during the active phase of TED.
Treatment Course
- 8 IV infusions given every 3 weeks (approximately 6 months total)
- First infusion 90 minutes; subsequent infusions 60 minutes if tolerated
- Average proptosis reduction: 2–3 mm (some patients see 5 mm or more)
- Approximately 83% of patients achieve meaningful proptosis reduction
- Diplopia improvement in approximately 68% of patients
Side Effects
- Hyperglycemia: Blood glucose monitoring is essential, especially in patients with diabetes or pre-diabetes; may require insulin or medication adjustment
- Hearing changes / tinnitus: Reported in some patients; may be related to IGF-1R blockade in the cochlea. Audiologic monitoring is recommended
- Muscle cramps, nausea, fatigue, hair loss, and infusion reactions (less common)
- Contraindicated in pregnancy — effective contraception required during treatment
Who Is a Candidate
- Active TED (CAS ≥ 3, evidence of inflammation) with moderate-to-severe disease
- TRAb/TSI positive (predicts better response)
- Best results within the first 9–12 months of TED onset
- Patients who have failed or cannot receive systemic corticosteroids
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.