
Eyelid Laxity
Treatment of lax or loose eyelids — ectropion, entropion, floppy eyelid syndrome — causing discomfort, tearing, or corneal exposure.
Patient Education Video
Dr. Brown explains common eyelid malpositions including ectropion and entropion — causes, symptoms, and surgical correction.
Eyelid Laxity

Description/Introduction
- Eyelids protect your eyes from any foreign bodies while keeping them lubricated throughout. Any alteration in the shape, position or function of your eyelids can predispose your eyes to a plethora of ailments or interfere with our vision.
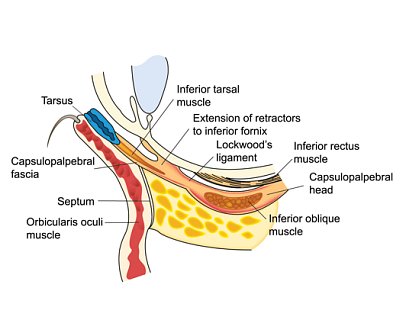
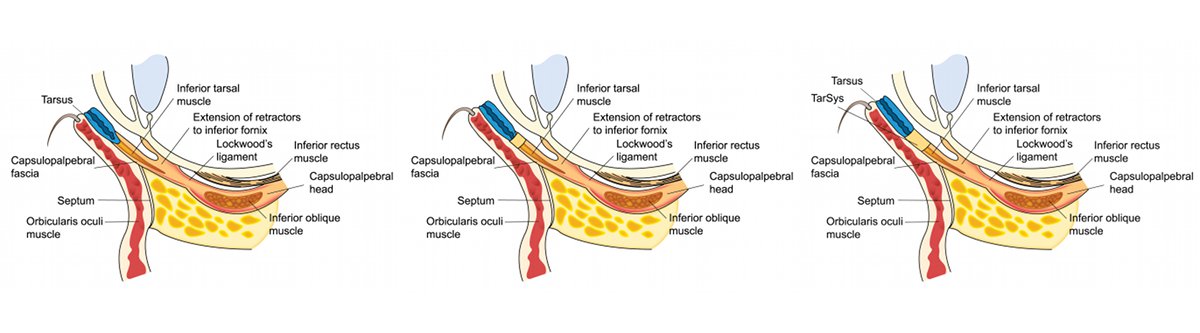
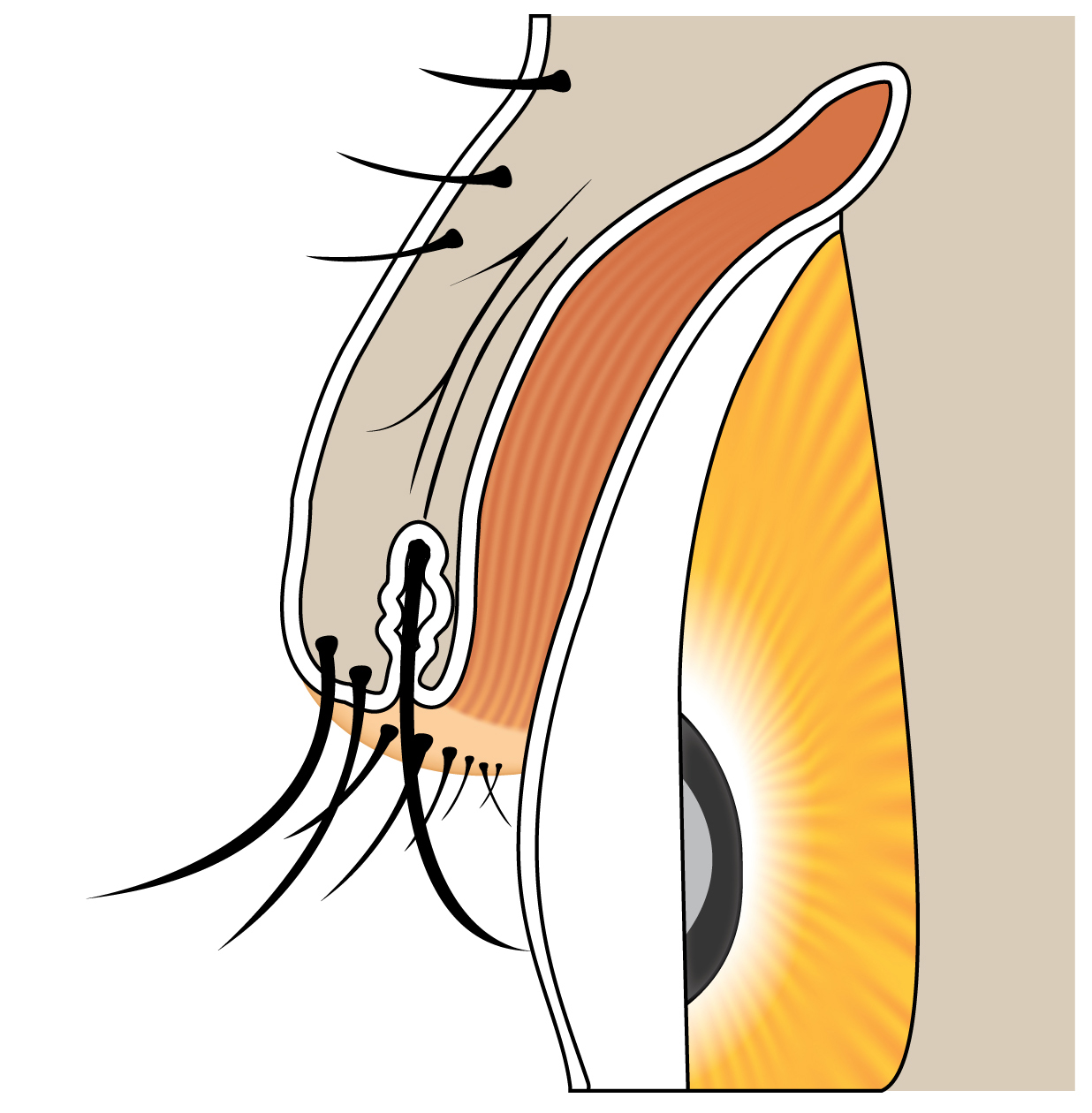
- Our eyelid is a complex structure consisting of three theoretical layers:
- Anterior Layer contains the skin and orbicularis muscle
- Middle Layer contains the orbital septum and eyelid retractors
- Posterior Layer contains tarsus and conjunctiva.
- Eyelid malpositions include any unnatural or incorrect positioning and orientation of eyelids due to various factors that influence any of the three layers of the eyelids. They may be caused due to ageing, trauma, scarring, birth defects or medical disease involving any or all of the three layers.
- The most common forms of eyelid malposition are eyelid retraction, ptosis, entropion and ectropion.
Types of Eyelid Malpositions
- Upper eyelid malpositions: Upper lid ptosis (drooping down of upper eyelid), retraction of the upper eyelid (causing apparently bulging eyes), entropion (in-turning of eyelid and lash line) and ectroprion (out-turning of the eyelid)
- Lower eyelid malpositions: Retraction of lower eyelid (lid margin below inferior limbus), entroprion (inward rotation of the eyelid margin) and ectroprion (outward rotation of the eyelid margin)
Common Consequences of Eyelid Malpositions
- Decreased vision due to blockage of visual axis by the mal-positioned eyelid or secondary to corneal ulcer formation.
- Irritation of the eyes due to an eyelash rubbing the cornea or conjunctiva
- Corneal ulcer due to repeated rubbing of corneal surface by the eyelashes or eyelid margin.
- Corneal or conjunctival dryness due to exposure leading to irritation, discomfort, keratitis or corneal ulcer.
- Repeated infections of the lachrymal sac due to a blocked punctum.
Common Symptoms associated with Eyelid Malpositions
- Dry eye and irritation
- Painful eye
- Disfigurement of the eyes
- Excessive watering of eyes
- Corneal ulcer
- Photophobia
- Decreased vision due to visual axis blockage by eyelids or corneal ulcer
- Disfigurement
Evaluation and treatment of eyelid malpositions needs to be disease-specific and tailored to the patient’s needs. This requires consultation with an eye surgeon familiar with treating various eyelid malpositions. More detailed explanations on each particular eyelid malposition is provided elsewhere for your ready reference
Eyelid Positional Disorders
Ectropion
Ectropion is the medical term used to describe sagging and outward turning of the lower eyelid and eyelashes. The margin of the eyelid and the eyelashes revert (turn out) . This rubbing can lead to excessive tearing, crusting of the eyelid, mucous discharge and irritation of the eye
Entropion
Entropion is the medical term used to describe sagging and outward turning of the lower eyelid and eyelashes. The margin of the eyelid and the eyelashes invert (turn in) . This rubbing can lead to excessive tearing, crusting of the eyelid, mucous discharge and irritation of the eye
Eyelash Disorders
Trichiasis: Lashes pointing to the eye
Other Eyelid conditions
Floppy Eyelid Syndrome: Eyelid sponanteously inverts
For a detailed guide to eyelid anatomy, see our dedicated Eyelid Anatomy page.
Ectropion
Ectropion is the outward turning of the lower eyelid margin away from the eye. When the lid no longer contacts the globe, tears cannot drain normally and the exposed conjunctiva becomes chronically irritated and inflamed.
Symptoms
- Excessive tearing and watery eyes
- Eye redness, irritation, and burning sensation
- Mucous discharge and eyelid crusting, especially in the morning
- Sensitivity to light and wind
- Risk of corneal damage from chronic exposure if untreated
Types of Ectropion
- Involutional (age-related) — the most common type, caused by gradual relaxation and horizontal laxity of the eyelid tendons and supporting tissue. Treated with lateral canthoplasty or a full-thickness lid-shortening procedure.
- Cicatricial — caused by scarring of the outer eyelid skin from burns, trauma, skin cancer, radiation, or chronic inflammatory skin conditions such as rosacea, eczema, or herpes zoster. Treatment restores vertical lid height, often with a skin graft.
- Paralytic — caused by weakness of the orbicularis muscle from facial nerve (CN VII) palsy due to Bell’s palsy, acoustic neuroma, or parotid or temporal bone tumors. Options include lubricating drops, a gold weight implant to aid eyelid closure, lower lid sling, or lateral tarsorrhaphy.
- Mechanical — a mass or growth physically pulling the eyelid away from the globe.
- Punctal ectropion — outward displacement limited to the tear drainage opening (punctum), causing chronic tearing even when the overall lid position appears normal.
Surgical Treatments
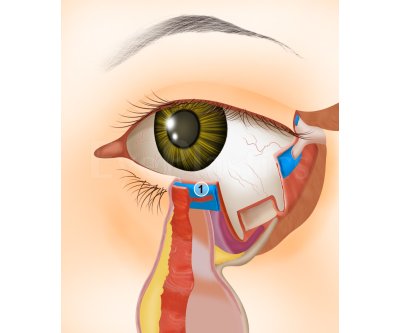
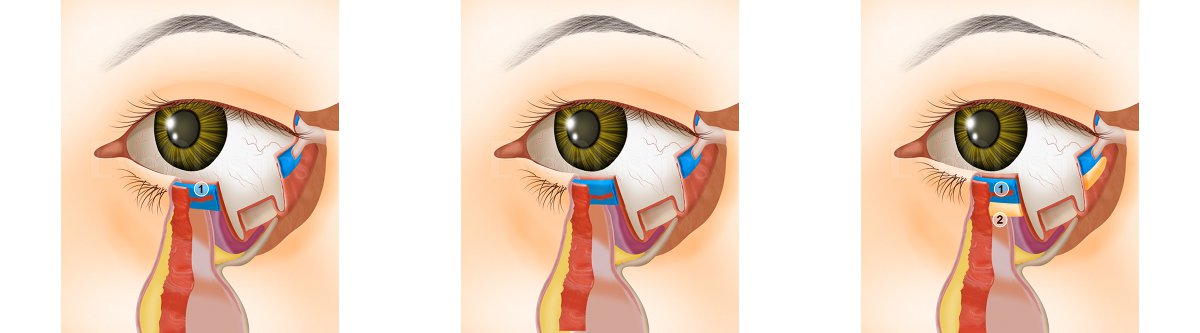
Lower Eyelid Retraction Correction — Surgical Animation
Interactive animation covering lower eyelid retraction anatomy and both the External and Internal surgical correction approaches.
Entropion

Entropion is the inward turning of the eyelid margin, causing eyelashes to rub against the cornea and conjunctiva. This chronic friction produces persistent irritation, tearing, redness, and — if left untreated — corneal scarring and vision loss.
Four Anatomic Factors That Cause Entropion
- Horizontal lid laxity
- Disinsertion or weakening of the lower eyelid retractors
- Preseptal orbicularis overriding the pretarsal orbicularis, rolling the lid margin inward
- Enophthalmos (sunken globe)
Types of Entropion
- Involutional (age-related) — the most common form, caused by retractor dehiscence, horizontal lid laxity, and orbicularis override. Corrected surgically with retractor re-attachment, tarsal strip, or horizontal lid shortening.
- Cicatricial — caused by scarring of the inner eyelid surface from trachoma, Stevens-Johnson syndrome, chemical burns, ocular cicatricial pemphigoid, or prior surgery. Treated with mucous membrane grafting, lamellar rotation, or scleral grafts.
- Acute spastic — triggered by ocular inflammation or irritation. Often resolves when the underlying cause is treated; Quickert sutures provide temporary relief.
- Congenital — rare; should be distinguished from epiblepharon. Treated by excising a small strip of skin and orbicularis below the lid margin.
Treatment Options
- Quickert sutures (temporary, office procedure)
- Thermal cautery (temporary)
- Lower eyelid retractor re-attachment
- Horizontal lid shortening (tarsal strip procedure)
- Full-thickness lid-splitting and marginal rotation
- Mucous membrane graft (cicatricial cases)
Floppy Eyelid Syndrome

Overview
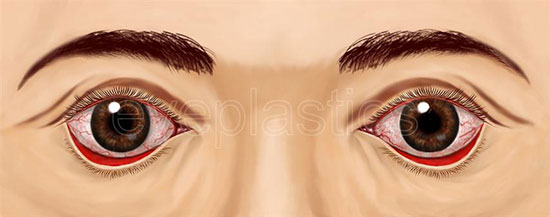
- A relatively uncommon condition characterized by loose, easily everted upper eyelids. Floppy eyelid syndrome (FES) is often seen in overweight, middle-aged males. Some of these patients also suffer from obstructive sleep apnea (OSA).
- Treatment for FES often includes artificial tears to reduce irritation and an antibiotic if signs of infection are present. Using tape or an eyeshield to keep the eyelids closed while sleeping may help prevent lid eversion and keep the eyes from becoming dry
- Symptoms generally consist of ocular injection, irritation, itching and stringy mucous discharge, particularly upon awakening. The symptoms may appear unilaterally or asymmetrically. Patients with OSA may also complain of erratic sleep patterns, chronic somnolence and morning headaches
- Examination of patients with FES typically reveals chronic papillary conjunctivitis with mild to moderate bulbar hyperemia, often lateralizing to the patient's habitual sleeping side (i.e., if they sleep on their left side, the presentation is more evident O.S.). Punctate corneal epitheliopathy and mucous strands in the tear film and fornices may also be apparent. The lids themselves routinely display pseudoptosis and an odd "rubbery" consistency. Eversion of the upper lids can be accomplished with minimal manipulation; in fact, it may occur spontaneously during normal ocular examination. Past ocular history may include meibomian gland dysfunction, hordeola or chalazia, keratoconus, and seasonal allergic conjunctivitis
Pathophysiology
- The etiology of FES is not thoroughly understood. Research has demonstrated that tarsal elastin is significantly diminished in these patients, such that the tarsal plate of the eyelid no longer displays its customary rigidity.4 One study suggests that individuals with FES may actually have underlying genetic collagen or elastin abnormalities.5
- The precise mechanism of this disorder also remains disputed. The most widely held theory suggests that, because of the lid laxity and tendency of these patients to lie on their sides or in a "face-down" position, spontaneous lid eversion occurs during sleep. This results in mechanical abrasion of the ocular surface. Others have suggested that the underlying mechanism is simply poor apposition of the upper eyelid to the globe, instigating an inadequate tear distribution and subsequent desiccation of the ocular surface
Management
- In the majority of cases, diagnosis is made by the classic appearance and effortless or spontaneous eversion of the eyelids. There are few ancillary tests to consider beyond the normal ocular evaluation, though vital dye staining (e.g., sodium fluorescein, rose bengal and/or lissamine green) may help to assess the severity of any associated keratopathy.
- Treatment for FES consists primarily of lubricating the ocular surface and safeguarding the eye from nocturnal damage. Isotonic artificial tears, used liberally throughout the day, help to eliminate mucous debris and promote corneal healing. In cases of moderate or profound epitheliopathy, consider more viscous lubricants such as Systane or Refresh Liquigel on a qid basis. At bedtime, the patient should instill either a bland ophthalmic ointment (e.g. Tears Naturale P.M.) or mild antibiotic ointment and apply a protective eye shield, or simply tape the lids in a closed position. Severe, recalcitrant cases that do not respond to primary therapy may require surgical intervention. Most commonly, this involves a lateral eyelid tightening procedure at the lateral canthus, or a horizontal lid shortening procedure by full-thickness resection of the lateral one-third of the lid margin.67 Lateral tarsorrhaphy has been suggested for noncompliant patients with severe disease.
- As important as managing the ocular sequelae of FES is addressing the associated problem of obstructive sleep apnea. OSA is a potentially fatal condition that has been linked to pulmonary hypertension, congestive heart failure and cardiac arrhythmia. Weight loss and consultation with a sleep physician for appropriate studies are highly recommended, considering the significant comorbidities of both obesity and OSA. At least one study has demonstrated notable improvement of FES when OSA is properly addressed.
Clinical Pearls
- Many patients with FES manifest attendant blepharitis, particularly meibomian gland dysfunction. Rosacea has also been found in association with both FES and OSA. Strongly consider a trial of oral doxycycline 100mg bid for six to 12 weeks.
- When interviewing patients with FES, always remember to inquire about prominent snoring or gasping episodes during sleep. In this regard, realize that a spouse or family member may actually prove to be a more reliable resource than the patient! Any such findings consistent with OSA warrant consultation with a sleep physician, otolaryngologist or pulmonologist.
References.
McNab AA. Floppy eyelid syndrome and obstructive sleep apnea. Ophthal Plast Reconstr Surg 1997;13(2):98-114. Mojon DS, Goldblum D, Fleischhauer J, et al. Eyelid, conjunctival, and corneal findings in sleep apnea syndrome. Ophthalmology 1999;106(6):1182-5. Robert PY, Adenis JP, Tapie P, et al. Eyelid hyperlaxity and obstructive sleep apnea (O.S.A.) syndrome. Eur J Ophthalmol 1997;7(3):211-5. Netland PA, Sugrue SP, Albert DM, et al. Histopathologic features of the floppy eyelid syndrome. Involvement of tarsal elastin. Ophthalmology 1994; 10(1)1:174-81. Lee WJ, Kim JC, Shyn KH. Clinical evaluation of corneal diseases associated with floppy eyelid syndrome. Kor J Ophthalmol 1996;10(2):116-21. Periman LM, Sires BS. Floppy eyelid syndrome: A modified surgical technique. Ophthal Plast Reconstr Surg 2002;18(5):370-2. Bouchard CS. Lateral tarsorrhaphy for a noncompliant patient with floppy eyelid syndrome. Am J Ophthalmol 1992;114(3):367-9. McNab AA. Reversal of floppy eyelid syndrome with treatment of obstructive sleep apnoea. Clin Experiment Ophthalmol 2000;28(2):125-6.
Trichiasis
Trichiasis describes misdirected eyelashes that grow toward the eye instead of away from it. Distichiasis is a separate condition in which a second row of lashes grows from the meibomian gland openings along the lid margin.
Trichiasis — Lashes pointing to the eye

Distichiasis
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.