Trauma
Surgical repair of eyelid, orbital, and lacrimal trauma — from minor lacerations to complex orbital fractures and reconstruction.
Periocular Trauma
Periocular trauma encompasses injuries to the eyelids, orbit, and lacrimal system. Because the eyelids protect the globe and the orbit houses the optic nerve, even apparently minor periocular trauma can have significant visual consequences. The initial priority in any periocular trauma is to rule out globe injury before proceeding with eyelid or orbital repair. A ruptured globe requires urgent ophthalmologic evaluation; wound exploration should be deferred until the globe is assessed and protected.
For a detailed review of orbital anatomy — bones, walls, foramina, and contents — see our dedicated Orbital Anatomy page.
Orbital Floor Fractures
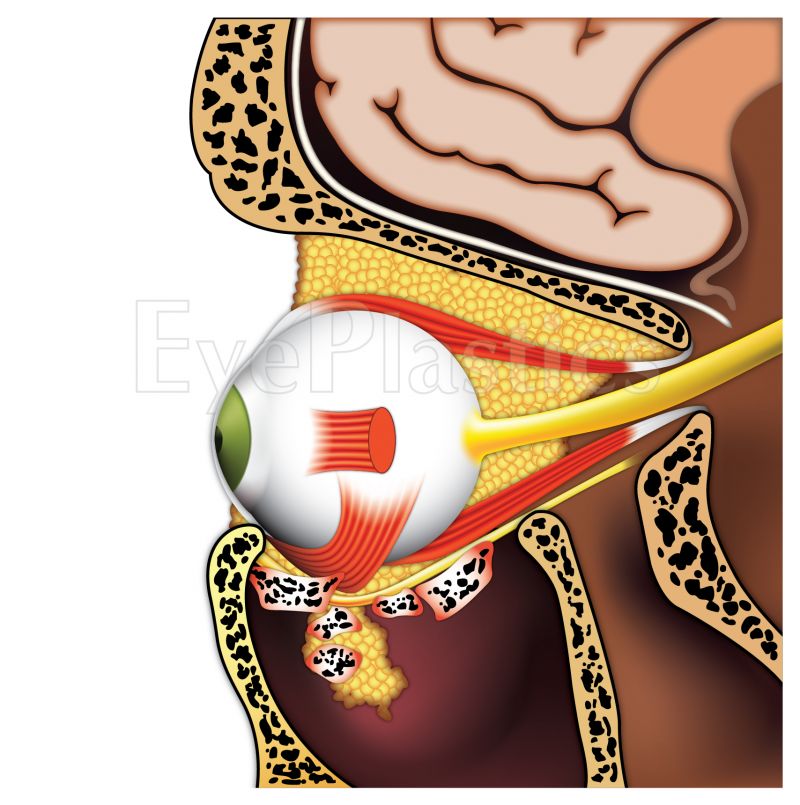
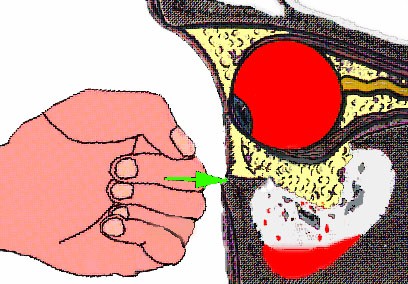
Orbital floor fractures result from blunt trauma to the periorbital region. The orbital floor (the roof of the maxillary sinus) is the thinnest bone in the orbit and fractures most commonly, followed by the medial wall adjacent to the ethmoid sinus. When force is applied to the orbit, intraorbital pressure rises acutely, causing the weakest wall to fracture outward into the adjacent sinus — a decompression mechanism that may protect the globe from more serious injury.
Published Research — Dr. Brown
Brown MS. Concomitant Ocular Injuries with Orbital Fractures. Dr. Brown’s research highlights the importance of comprehensive ocular evaluation at the time of orbital fracture presentation, as globe injuries frequently occur alongside orbital fractures and may be missed on initial assessment.
Types of Orbital Fractures
- Pure blowout fracture — fracture limited to the orbital walls without rim involvement; the rim remains intact. Most commonly involves the floor or medial wall. Fat and occasionally muscle herniate into the adjacent sinus.
- Orbital rim fracture — fracture involves the orbital rim itself; often associated with zygomaticomaxillary complex (ZMC) fractures, frontal sinus fractures, or LeFort patterns.
- Trapdoor fracture — a greenstick variant most common in children; the bone flexes and snaps back, trapping orbital contents within the fracture. Children may have minimal external signs yet present with severe restriction of upgaze, nausea, and bradycardia (“oculocardiac reflex”). This constitutes a surgical emergency — urgent repair within 24–48 hours is required to prevent ischemic contracture of the entrapped inferior rectus muscle.
Clinical Findings
- Enophthalmos — posterior displacement of the globe from increased orbital volume; may be delayed 2–4 weeks as edema resolves
- Hypoglobus — downward displacement of the globe with large floor fractures
- Diplopia — from muscle entrapment, direct muscle injury, or periorbital edema restricting eye movement; most resolves spontaneously as swelling decreases
- Infraorbital nerve hypoesthesia — numbness of the cheek, lower lid, and upper gum from injury to the infraorbital nerve as it traverses the orbital floor
- Subcutaneous emphysema — air in periorbital tissues from sinus communication; patients should be instructed not to blow their nose
- Periorbital ecchymosis and edema — bilateral periorbital bruising (“raccoon eyes”) with orbital rim fractures may suggest a skull base fracture
Imaging
CT of the orbits in coronal and axial planes with bone and soft-tissue windows is the study of choice. The coronal view best demonstrates floor and medial wall fractures and muscle entrapment. CT findings guide surgical planning: fracture size and location, degree of fat or muscle herniation, and presence of bone fragments within the sinus.
Surgical Indications and Timing
Not all orbital fractures require surgery. Repair is indicated for:
- Symptomatic diplopia persisting beyond 2 weeks without improvement, particularly with a positive forced duction test confirming mechanical entrapment
- Clinically significant enophthalmos (>2 mm) or hypoglobus causing functional or cosmetic concern
- Large floor fracture (>50% of the orbital floor) predicting late enophthalmos, even without current symptoms
- Trapdoor fracture with muscle entrapment — urgent repair within 24–48 hours
For non-emergency fractures, most surgeons prefer to wait 10–14 days to allow edema to resolve before repair. The orbital floor is typically accessed through a transconjunctival incision (invisible scar). Herniated contents are reduced and the fracture is covered with a reconstruction plate — porous polyethylene, titanium mesh, or resorbable material depending on defect size.
Lacrimal Trauma
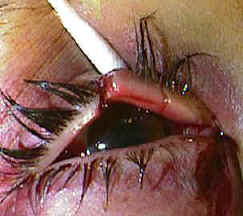

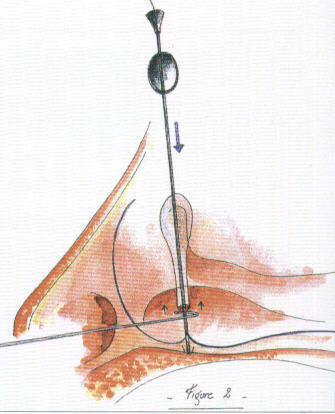
Canalicular lacerations result from trauma to the medial eyelid — commonly from dog bites, fingernail injuries, or blunt trauma that avulses the medial canthal region. The lower canaliculus carries approximately 70% of tear drainage, making lower canalicular lacerations more functionally significant. Any laceration medial to the punctum should be evaluated for canalicular involvement by slit-lamp exam or probing under magnification.
Primary repair with silicone stent intubation is performed within 24–48 hours when possible. The stent maintains the canalicular lumen while healing occurs and is removed at 3–6 months. When both canaliculi are severed or the lacrimal sac is disrupted, dacryocystorhinostomy (DCR) may be required to restore drainage. See the Lacrimal System page for detailed information on repair technique and anatomy.
Eyelid Lacerations

Eyelid lacerations are classified by depth (partial vs. full-thickness), involvement of the lid margin, and canalicular involvement. Eyelid tissue has excellent vascularity — even tissue that appears devitalized should be preserved whenever possible.
Evaluation
- Globe injury must be excluded first — do not probe wounds or apply pressure until globe assessment is complete
- Lid margin involvement — any laceration through or near the gray line requires careful layered repair to prevent notching, trichiasis, or entropion
- Medial lacerations — any laceration medial to the punctum should be assumed to involve the canaliculus until proven otherwise
- Fat visible in wound — indicates penetration through the orbital septum; orbital fat prolapse signals potential posterior injury
- Ptosis at presentation — may indicate levator aponeurosis injury requiring repair at the time of laceration closure
Repair Principles
- Copious irrigation and debridement of debris; antibiotic prophylaxis for contaminated wounds
- Full-thickness lid lacerations are repaired in layers: tarsal plate (posterior lamella) first, then skin and orbicularis (anterior lamella); the lid margin requires precise alignment of the gray line, mucocutaneous junction, and lash line to prevent notching or misdirected lashes
- Tissue avulsion — even small bridges of attached tissue should be preserved; significant tissue loss may require staged reconstruction with advancement flaps or grafts
- Dog bites cause significant crush and avulsion injury; antibiotic prophylaxis covering Pasteurella multocida and Capnocytophaga is essential; primary repair is generally possible due to excellent eyelid vascularity
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.