Ptosis vs. Blepharoplasty: Which Eyelid Condition Do You Have?
The correct diagnosis determines the treatment — and whether insurance will cover it.
Ptosis — Drooping Eyelid Margin
The eyelid edge (margin) sits too low — partially covering the pupil. Caused by weakness or disinsertion of the levator muscle. The overlying skin may look completely normal.
Treatment: muscle surgery (ptosis repair)
Blepharoplasty — Excess Eyelid Skin
The eyelid margin is in its normal position, but excess skin (dermatochalasis) hangs over it — creating a heavy, tired appearance. The lifting muscle works normally.
Treatment: skin and fat removal
What Each Condition Looks Like
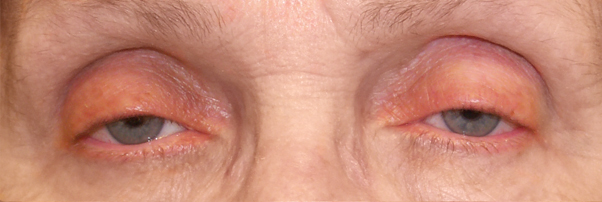
Ptosis — eyelid margin droops over the pupil
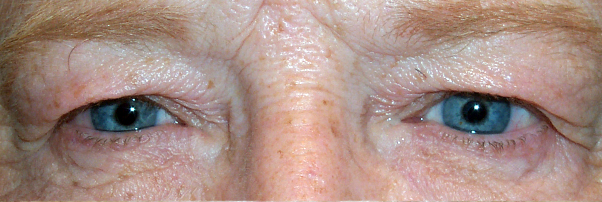
Dermatochalasis — excess skin hoods over normal lid margin
A Simple Self-Assessment
Stand in front of a mirror in good lighting. Look straight ahead — do not raise your brows.
1. When looking straight ahead — without raising your brows — does the upper eyelid cover part of your pupil?
If yes: this suggests ptosis. The eyelid margin itself sits too low.
2. Does excess skin hang over your upper eyelid, but the eyelid edge (near the lashes) appears to sit at a normal height?
If yes: this suggests dermatochalasis — you may be a blepharoplasty candidate.
3. Do you find yourself unconsciously raising your eyebrows throughout the day to see clearly, or tilting your chin up?
If yes: this compensation pattern occurs with both ptosis and excess skin — evaluation is needed.
4. Does the drooping worsen noticeably as the day progresses or after sustained reading?
If yes: fluctuating ptosis may indicate myasthenia gravis — a neurologic cause that must be excluded before any surgery.
Ptosis in Detail
Ptosis (pronounced TOE-sis) is drooping of the upper eyelid caused by weakness, stretching, or disinsertion of the levator palpebrae superioris — the muscle responsible for lifting the upper eyelid. Müller's muscle, the secondary elevator, may also be involved.
Common Causes
- Involutional (age-related): the most common — the levator tendon stretches or detaches over time
- Contact lens–related: chronic mechanical irritation from lens insertion and removal
- Post-surgical: following cataract surgery, LASIK, or any procedure requiring a lid speculum
- Horner's Syndrome: mild ptosis with miosis (small pupil) — may indicate a serious underlying cause requiring imaging
- Third Nerve (CN III) Palsy: significant ptosis often with double vision and a dilated pupil — urgent evaluation required
- Myasthenia Gravis: fluctuating, fatigue-dependent ptosis — must be excluded before surgical planning
- Congenital: present from birth — requires early evaluation to prevent amblyopia (lazy eye)
Surgical Treatment Options
- Levator advancement: the most common repair — the levator aponeurosis is tightened through an incision in the eyelid crease
- Müller's muscle–conjunctival resection (MMCR): for mild ptosis with good levator function; predictable results when the phenylephrine test is positive
- Frontalis suspension: for severe ptosis with poor levator function — the eyelid is suspended using a sling attached to the brow muscle
- Upneeq® (oxymetazoline 0.1%): prescription drops that temporarily lift the eyelid 1–2 mm; for mild ptosis or patients avoiding surgery
Insurance Coverage
Ptosis repair is frequently covered by insurance when it causes visual impairment — typically demonstrated by superior visual field loss ≥12 degrees on Humphrey or Goldmann perimetry. Medical photos, visual field results, and margin reflex distance measurements are required for preauthorization.
Blepharoplasty (Excess Eyelid Skin) in Detail
Blepharoplasty candidates typically have dermatochalasis — accumulated excess skin of the upper eyelid caused by aging, sun exposure, and hereditary factors. The levator muscle functions normally; the problem is in the tissue above it.
What Blepharoplasty Addresses
- Excess upper eyelid skin that hangs over the lash margin (dermatochalasis)
- Herniated orbital fat creating fullness in the medial upper eyelid or lateral brow area
- Lower eyelid fat bags (pseudoherniated fat) and redundant skin
- Heavy, tired appearance from skin overhanging the eyelid crease
What Blepharoplasty Does NOT Correct
- A low eyelid margin (ptosis) — skin removal may unmask underlying ptosis
- Brow ptosis — a descended brow will continue overhanging the eyelid after upper blepharoplasty
- Festoons or malar mounds on the lower cheek (different anatomy, different treatment)
Insurance Coverage
Upper blepharoplasty may be covered when excess skin obstructs the superior visual field, documented by visual field testing performed with and without the skin lifted. Clinical photographs showing skin resting on or below the lash margin are typically required for prior authorization.
When Both Are Present: The Combined Case
It is common — particularly in patients over 55 — to have both dermatochalasis and involutional ptosis simultaneously. Treating only one produces a suboptimal result:
- Blepharoplasty alone in a patient with unrecognized ptosis may “unmask” the drooping — removing the weight of excess skin reveals the margin is actually lower than expected
- Ptosis repair alone when significant dermatochalasis exists may leave the patient with persistent skin heaviness and incomplete improvement
When both conditions are identified preoperatively, Dr. Brown addresses them in a single operative session, minimizing recovery time and anesthesia exposure.
Ready for an Evaluation?
A thorough examination — including measurement of the eyelid margin position, levator function, and visual field assessment — is the only reliable way to distinguish ptosis from dermatochalasis. Dr. Brown evaluates both in a single consultation.