Orbital Tumors
Diagnosis and surgical management of orbital tumors and masses — adult and pediatric, benign and malignant.
Orbital Bones — Interactive Anatomy
Click on any bone or foramen in the diagram to identify the seven bones and foramina that make up the orbit.

Click any region to identify the orbital bones and foramina.
Orbital Muscles — Interactive Anatomy
Click any marker to identify the six extraocular muscles, the levator palpebrae, and surrounding orbital structures.
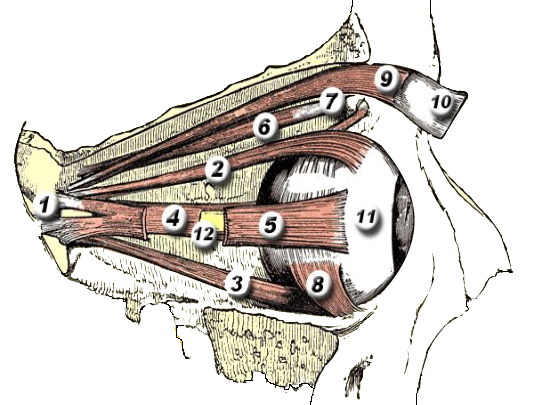
Click any marker to identify the extraocular muscles.
Orbital Tumors

The orbit is a bony cavity approximately 30 mL in volume that houses the eye, six extraocular muscles, the optic nerve, fat, lacrimal gland, and a rich network of blood vessels and nerves. A tumor — any space-occupying lesion, benign or malignant — within this confined space produces characteristic signs by displacing or compressing orbital contents.
Most orbital tumors are benign. The clinical priority is accurate characterization — imaging-guided diagnosis avoids unnecessary surgery for lesions that can be observed, while ensuring timely biopsy and treatment for malignancies. Dr. Brown performs orbital biopsy and surgical excision; for tumors requiring neurosurgical or skull-base approaches, he coordinates care with neurosurgical colleagues.
For a detailed guide to orbital anatomy, see our dedicated Orbital Anatomy page.
Signs and Symptoms of Orbital Tumors
Orbital tumors produce symptoms by displacing the eye or compressing orbital structures. The direction of displacement helps localize the lesion:
- Proptosis (exophthalmos) — forward displacement of the globe; the most common sign of any space-occupying orbital lesion
- Axial vs. non-axial proptosis — lesions within the muscle cone (intraconal) push the eye straight forward (axial); extraconal masses displace the eye away from the tumor
- Double vision (diplopia) — from displacement of the globe or direct infiltration of extraocular muscles
- Visual loss — compression of the optic nerve; may be subtle initially (afferent pupillary defect, color desaturation)
- Pain — more common with rapidly expanding, inflammatory, or malignant lesions; slowly growing benign tumors are often painless
- Eyelid changes — fullness, ptosis, or an obvious mass at the orbital rim
- Palpable mass — particularly for anterior orbital tumors near the orbital rim
Urgent evaluation: Any rapidly progressive proptosis, vision loss, or pain requires prompt CT/MRI imaging and orbital evaluation. Childhood orbital masses deserve urgent assessment — rhabdomyosarcoma grows in days to weeks.
Diagnosis
CT and MRI are complementary — CT better demonstrates bony involvement and calcification; MRI provides superior soft-tissue characterization and optic nerve detail. The shape, location, density/signal, and enhancement pattern of the lesion often suggest the diagnosis before biopsy. Fine-needle aspiration biopsy (FNAB) or incisional biopsy under imaging guidance provides tissue for pathology when clinical diagnosis is uncertain.
Common Adult Orbital Tumors

Cavernous Venous Malformation (Cavernous “Hemangioma”)
The most common primary orbital tumor in adults. Despite the historical name, it is a venous malformation — a well-encapsulated mass of enlarged vascular spaces within the muscle cone. It typically presents in women aged 30–60 with slowly progressive painless axial proptosis. CT shows a well-defined, homogeneously enhancing intraconal mass. MRI demonstrates progressive centripetal enhancement. Treatment is surgical excision when vision is threatened or proptosis is cosmetically significant; asymptomatic lesions can be observed.
Hemangiopericytoma (Solitary Fibrous Tumor)

Solitary fibrous tumor / hemangiopericytoma is a mesenchymal tumor of perivascular cells that can arise anywhere in the orbit. It is less well-encapsulated than cavernous hemangioma and may have locally invasive behavior. Complete surgical excision is the treatment of choice; incomplete excision leads to recurrence. A subset of cases behaves aggressively with distant metastasis. Pathologic grading (WHO) guides adjuvant treatment decisions.
Lacrimal Gland Tumors
The lacrimal gland, located in the superolateral orbit, gives rise to a spectrum of lesions. The clinical rule of “50/50” applies: approximately 50% of lacrimal gland masses are epithelial neoplasms and 50% are inflammatory or lymphoid. Of the epithelial tumors, 50% are benign mixed tumors (pleomorphic adenoma) and 50% are malignant.
- Pleomorphic adenoma — the most common lacrimal gland epithelial tumor; presents over months to years with painless superolateral orbital fullness and downward-inward displacement of the globe. CT shows a well-defined fossa scalloping the lacrimal gland fossa. Complete excision with intact pseudocapsule is mandatory — capsule rupture or piecemeal removal risks recurrence and malignant transformation to carcinoma ex pleomorphic adenoma
- Adenoid cystic carcinoma — the most common malignant lacrimal gland tumor; characterized by perineural invasion and pain. Presents more rapidly than pleomorphic adenoma, often with pain. Despite aggressive treatment (exenteration + radiation), recurrence rates are high and prognosis is poor. High index of suspicion is warranted for any painful, rapidly progressive lacrimal gland mass
- Dacryoadenitis — inflammatory swelling of the lacrimal gland from infection (acute: Staphylococcus, gonorrhea; chronic: sarcoidosis, IgG4-related disease, sjögren’s)
Orbital Lymphoma


Orbital lymphoma is the most common malignant orbital tumor in adults over 60, accounting for 10–15% of all orbital tumors. Most are B-cell non-Hodgkin lymphomas, predominantly extranodal marginal zone lymphoma (EMZL, also called MALT lymphoma). Orbital and conjunctival lymphoma may be the initial presentation of systemic disease or may arise as a primary ocular adnexal tumor.
Clinical features: Painless, slowly progressive proptosis, lid swelling, or salmon-colored conjunctival mass. The classic imaging finding is a mass that “molds” around orbital structures without bone erosion — reflecting the lymphoma’s soft consistency.
Management: Biopsy followed by systemic staging workup (CT chest/abdomen/pelvis, bone marrow biopsy). Low-grade localized orbital EMZL is treated with low-dose external beam radiation (24 Gy) with >90% local control. Systemic or high-grade disease requires chemotherapy (R-CHOP); anti-CD20 therapy (rituximab) is used for B-cell lymphomas.
Neurofibroma and Plexiform Neurofibroma
Orbital neurofibromas may be solitary or plexiform. Plexiform neurofibroma is pathognomonic of Neurofibromatosis type 1 (NF-1) and involves the periorbital and orbital tissues diffusely. It presents in childhood as a “bag of worms” soft tissue mass with S-shaped ptosis and the classic NF-1 “absent greater wing of sphenoid” on imaging (pulsating proptosis due to bony defect). Management is challenging — surgical debulking reduces volume but complete resection is impossible; MEK inhibitor therapy (selumetinib) is now FDA-approved for pediatric plexiform neurofibromas.
Orbital Schwannoma
Schwannomas arise from the Schwann cells of peripheral nerves and are well-encapsulated, slow-growing tumors. In the orbit, they typically arise from peripheral branches of the trigeminal nerve (CN V) and present as painless, slowly progressive proptosis over years. CT shows a well-defined, enhancing mass. Surgical excision with preservation of the nerve capsule is curative; the capsule plane allows safe dissection.
Sphenoid Wing Meningioma
Meningiomas arising from the sphenoid wing invade the orbit through the superior orbital fissure or directly through bone, producing progressive proptosis, visual loss, and motility restriction. The “en plaque” variant grows as a flat sheet along the bone rather than a discrete mass. CT characteristically shows hyperostosis (bony thickening) of the sphenoid wing — a distinctive feature not seen with orbital lymphoma or metastases.
Management is complex, often requiring multidisciplinary planning with neurosurgery. Surgical decompression is indicated for progressive visual loss; total resection is rarely achievable given the infiltrative growth. Stereotactic radiosurgery (Gamma Knife) provides tumor control for smaller lesions. Observation is appropriate for asymptomatic or slowly progressive disease in older patients.
Common Pediatric Orbital Tumors
The differential diagnosis of orbital masses in children differs substantially from adults. Most pediatric orbital tumors are benign developmental lesions, but rhabdomyosarcoma — the most common malignant orbital tumor of childhood — must always be considered in any rapidly growing mass.
Capillary Hemangioma (Infantile Hemangioma)



Infantile hemangiomas are the most common periorbital tumors of infancy, arising from proliferating vascular endothelium. They are absent or faint at birth, proliferate rapidly in the first 6–12 months, then involute slowly over years (50% by age 5, 70% by age 7, 90% by age 9). Most require only observation.
Indications for treatment: Obstruction of the visual axis causing deprivation amblyopia, astigmatism from lid pressure on the cornea, significant proptosis from a deep orbital component, or ulceration.
Propranolol is the first-line treatment — oral propranolol (1–3 mg/kg/day) produces rapid and reliable involution by causing vasoconstriction, reduced VEGF expression, and increased apoptosis of hemangioma endothelium. Topical timolol 0.5% gel is used for superficial lesions. Steroid injection and surgical excision are now second-line options.
Dermoid Cysts
Dermoid cysts are the most common orbital masses of childhood and the most common benign orbital tumor overall. They are choristomas (normal tissue in an abnormal location) — epithelially lined cysts containing keratin, hair, and sebaceous material that arise at sutural lines from trapped ectoderm during embryonic development. The classic location is the superolateral orbital rim (frontozygomatic suture), presenting as a smooth, non-tender, mobile mass in a child.
Dermoids do not involute. They are excised electively — typically before school age. Complete excision with an intact cyst wall is essential: rupture of the cyst spills highly irritating contents and causes severe granulomatous inflammatory reaction that makes complete removal difficult. Deep dermoids extending through the lateral orbital wall into the temporalis fossa require CT planning before surgery.
Lymphatic Malformation (Lymphangioma)
Lymphatic malformations are congenital vascular malformations of abnormally connected lymphatic channels. Unlike hemangiomas, they do not involute. They infiltrate orbital tissues diffusely and may expand suddenly (“hemorrhage into the cyst” — chocolate cysts) following upper respiratory infections or trauma, producing acute painful proptosis.
Management is challenging due to their infiltrative nature. Options include observation for stable lesions, sclerotherapy (OK-432 or doxycycline injection) for cystic components, and surgical excision for accessible components. Complete resection is rarely achievable. Sirolimus (mTOR inhibitor) has shown benefit in complex vascular malformations refractory to other treatments.
Schedule a Consultation
Contact us to discuss your concerns and learn about treatment options.